INTRODUCTION The temporomandibular joint (TMJ) is considered one of the most complete human being, as it allows various movements, such as opening, closing, protrusion, retrusion and lateral jaw (1). Temporomandibular disorders (TMD) comprise a series of clinical problems involving the masticatory muscles, the joint itself and associated structures (2, 3, 4, 5).
Studies have shown (6, 7, 8, 9) the absence of an etiological factor that is responsible for TMD, and is therefore a multifactorial disease, which includes factors traumatic degenerative problems, harmful habits, abnormal position of the condyle and the articular disc, excessive masticatory muscle activity and psychosocial variables and psychological.
Approximately 70-93% of the population in general, has at least one sign and / or symptoms of TMD, but only one in four people, has such knowledge (2, 10). Study conducted to verify the symptoms of TMD in 144 individuals (10) points out that only 5-13%, with more than one signal and / or symptoms of TMD, presents clinically significant change, such as pain or severe dysfunction.
The DTMs are characterized by a series of clinical signs and symptoms that manifest themselves as: muscle aches, headache, TMJ clicks, difficulties in performing mandibular movements, limiting the range of mandibular movements, especially with respect to mouth opening (4, 11 , 12, 13, 14, 15, 16, 17, 18).
These signals arise from inflammation of the area retrodiscal since the articular disc is displaced (6). The area retrodiscal to suffer stress can produce inflammation resulting in pain with continuous characteristic (19).
With regard to otological symptoms related to TMD, the most cited in the literature (20, 21), is the tinnitus, otalgia, ear fullness, hearing loss and vertigo.
The association of TMD and the origin of otologic symptoms, yet are not fully understood (4, 22, 24, 24). There are some hypotheses about the relationship between otological symptoms and TMD. The first is that poor positioning of the mandibular condyle could cause symptoms of otalgia, tinnitus and vertigo.
The buzz in TMD patients may be due to a neural signal induced by auriculo temporal nerve or reduction of sensory signals (2). This symptom may be due to other changes such as diseases of the inner ear or central nervous system (25).
If a reporter about trauma in the TMJ (26) mentions that the mandibular condyle to suffer a dislocation can cause a stretching of the ossicular chain and trigger aural symptoms.
Another hypothesis goes toward pointing which occurrence hyperactivity muscles mastication can contract muscle tensor tympani and membrane tympanic fact resulting in one dysfunction tubarius with symptoms Auricular fullness, imbalance and hearing loss (20, 24, 26, 27).
The study therefore aims to examine the relationship between TMD and otologic symptoms.
METHOD This research was approved by the Ethics in research on the subject. 04/803, and all participants signed an informed consent.
Study participants were 20 graduate students in speech pathology students, mean age 22.38 years who had previously conducted listening tests, ie, pure tone audiometry, speech audiometry and immittance.
All participants were assessed by a multidisciplinary team which includes ENT, speech therapists and orthodontists. The study participants were subjected to complete a questionnaire delivered by speech therapists who had questions related to symptoms of TMD and otological prepared for this research.
In the anatomy laboratory of the university, otoscopy was performed with the ENT doctor to verify the presence (when present visible fluid in the middle ear opacification, retraction and immobility of the tympanic membrane during inflation) or absence (full, translucent and with movement in insufflation) amendment.
Clinical examination was performed of the temporomandibular joint by an orthodontist, who collected data regarding the presence of TMD. There was pain in the muscles of mastication, clinical signs of TMD (crackling, clicking, and deviation of jaw movements) and presence of deleterious habits (bruxism, clenching teeth and onychophagy).
Statistical analysis considered the following data: the questionnaire was considered subject to change otological who self-reported at least one symptom of ear pain, ear fullness, tinnitus and vertigo: and dental evaluation, the TMD was defined by the presence of three or more signs and / or symptoms, therefore, essential symptom of pain.
All data were entered in an Excel spreadsheet and to measure the degree of relationship between otological symptoms and TMD was used Fisher's exact test, and significance level of 5%.
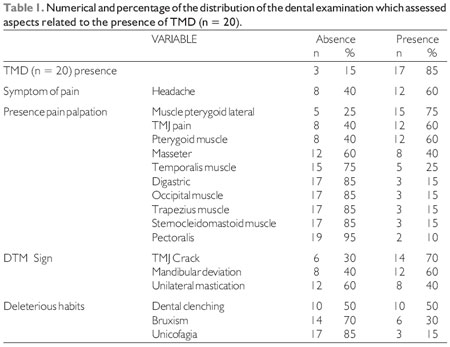
RESULTS Table 1 presents the data collected from the dental evaluation.
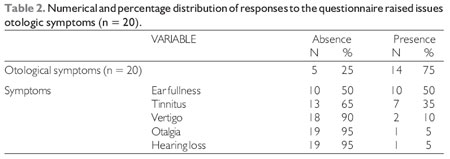
Table 2 presents the data gathered from the questionnaire and characterize the participants in the matters related to otologic symptoms.
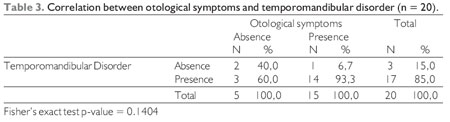
Table 3 presents the description of jaw movements and facial asymmetry in the evaluation of Orofacial.
In the Table 3 were explained the relationship and agreement between otological symptoms and TMD.
DISCUSSION This study sought a possible relationship between TMD and otologic symptoms. It was found in 85% of the presence of pain accompanied by two or more signs or symptoms for TMD. The DTMs are characterized by several signs and symptoms that manifest themselves in the orofacial muscles (2, 3, 4, 5) and pre-auricular region, near the ear (21).
The main signs and symptoms of TMD in this study are: crack (70%), deviation of jaw movements (60%), headache (60%) and pain on the TMJ (60%). Study constatou-if in TMD subjects, presence diversion mandible and vertical reduction mandibular movements (18). These problems may be triggered by factors involving occlusion abnormal position condyle Jaw, excessive activity musculature orofacial habits and psychosocial variables and psychological (7).
Pain to palpation was observed in muscles of mastication, especially the lateral pterygoid muscles (75%). This may be related to the fact that the pterygoid muscles, establish a direct relationship with the mandibular condyle and work together with the masseter and temporal muscles in the performance of mandibular movements (27). Study (6) mentions that the pain comes from inflammation or tension in the joint area.
The results of this study show no statistical correlation between otological symptoms and TMD (p = 0.1404). Of the 20 patients analyzed 17 (85%) had TMD and 15 (75%), otologic symptoms. Of these 15 patients with otologic symptoms, 14 (93, 3%) presented TMD. Thus, in patients with TMD (17), 85% also self-reported otologic symptoms.
Otologic symptoms more self-reported by the sample were of ear fullness and tinnitus. These symptoms have also been reported in the literature in patients with TMD (20, 23, 24, 26, 27).Otologic symptoms are associated with difficulties in jaw movements, open your mouth and the functions of the stomatognathic system (23) (chewing, swallowing, breathing and speaking).
It is important that focus should be alert to the symptoms of tinnitus, since such a change may be due to diseases of the inner ear or central nervous system and not only for TMD (25).
Research (26) suggests that the mandibular condyle to undergo a shift may cause stretching of the ossicular chain and thus the occurrence of otologic symptoms.
Another hypothesis goes toward pointing which occurrence hyperactivity muscles mastication, turn lead muscle contraction tensor tympanum and membrane tympanic or twitch velum.This may cause dysfunction of the Eustachian tube and in sequence, symptoms of ear fullness, imbalance and hearing loss (20, 24, 26, 27).
You could say that the relationship and origin of otologic symptoms have not yet been fully clarified (23). But search (24) proves that DTMs usually come associated otologic symptoms.
CONCLUSION The findings of this study indicate high prevalence of otologic symptoms in patients with TMD. We highlight the importance of research in the evaluation of otologic symptoms of TMD.It also suggested further research with larger samples of subjects to confirm the relationship between TMD and otologic symptoms.
BIBLIOGRAPHICAL REFERENCES1. Ilha VCA, Rapoport A, Filho JBI, Reis AA, Boni ASB. Estimativa da excursão condilar em pacientes com disfunção craniomandibular: um enfoque multidisciplinar. Rev Dent Press Ortodon Ortopedi Facial. 2006, 11(3):63-70.
2. Silvinelli F, Casale M, Paparo F, Persico AM, Zini C. Subjective tinnitus, temporomandibular joint dysfunction, and serotonin modulation of neural plasticity: causal or causal triad? Med Hypotheses. 2003, 61(4):444-448.
3. Ferrario VF, Tartaglia GM, Luraghi FE, Sforza C. The use of surface electromyography as a tool in differentiating temporomandibular disorders from neck disorders. Man Ther. 2006, 12(4):372-379.
4. Farella MA, Michelotti A, Bocchino T, Cimino R, Laino AMH, Steenks MH. Effects of orthognathic surgery for class III malocclusion on signs and symptoms of temporomandibular disorders and on pressure pain thresholds of the jaw muscles. Int J Maxilofac Oral Surg. 2007, 2(1):101-110.
5. Zocoli R, Mota EM, Sommavilla A, Perin RL. Manifestações otológicas nos distúrbios da articulação temporomandibular. ACM Arq Catarin Med. 2007, 36(1):90-95.
6. Takayama YDMD, Miura PHD, Yuasa DMD, Kobayashi K, Hosoi T. Comparison of occlusal condition and prevalence of bone change in the condyle of patients with and without temporomandibular disorders. Oral Radiol Endod. 2008, 105(1):104-112.
7. Proff P, Richter EJ, Blens T, Fanghanel J, Hutzen D, Korda B et al. A michigan-type occlusal splint with spring-loaded mandibular protrusion functionality for treatment of anterior disk dislocation with reduction. Ann Anat. 2007, 189(4):362-366.
8. Barbosa TS, Miyakoda LS, Pocztaruk RL, Gavião MBD. Temporomandibular disorders and bruxism in childhood and adolescence: Review of the literature. Int J Pediatr Otorhinolaryngol. 2008, 72(3):299-314.
9. Castrillon EE, Cairns BE, Ernberg M, Wangd K, Sessle B, Arendt-Nielsen L, Svensson P. Glutamate-evoked jaw muscle pain as a model of persistent myofascial TMD pain? Arch Oral Biol. 2008, 53(7):666-676.
10. Galdón MJ, Durá E, Andreu Y, Ferrando M, Poveda R, Bagán V. Multidimensional approach to the differences between muscular and articular temporomandibular patients: Coping, distress and pain characteristics. Oral Radiol. 2006, 102(1):40-46.
11. Scolozzi P MDDMD, Becker MMD, Richter MMDDMD. Temporomandibular Joint Osteoarthritis: A Cause of a Serous Otitis Media? A Case Report. J Oral Maxillofac Surg. 2004, 62(1):97-100.
12. Mariz ACR, Campos PSF, Sarmento VA. Avaliação dos deslocamentos de disco da articulação temporomandibular. Braz Oral Res. 2005, 19(1):63-68.
13. Elias FM, Birman EG, Matsuda CK, Oliveira IRS, Jorge WA. Ultrasonographic findings in normal temporomandibular joints. Braz Oral Res. 2006, 20(1):25-32.
14. Siqueira JTT, Ching LH, Nasri C, Siqueira SRDT, Teixeira MJ, Heirs G, Valle LBS. Clinical study of patients with persistent orofacial pain. Arq Neuropsiquiatr. 2004, 62(4):988-996.
15. Bianchini EMG, Paiva G, Andrade CRF de. Movimentos mandibulares na fala: interferência das disfunções temporomandibulares segundo índices de dor. Pró-fono. 2007, 19(1):7-18.
16. Felício CM de, Melchior MO, Silva MAMR, Celeghini RMS. Desempenho mastigatório em adultos relacionado com a desordem temporomandibular e com a oclusão. Pró-fono. 2007, 19(2):151-158.
17. Bianchini EMG. Mandibular movement patterns during speech in subjects with temporomandibular disorders and in asymptomatic individuals. J Craniomandibular Pract. 2008, 26(1):50-58.
18. Machado IM. Bianchini EMG. Andrada e Silva MA. Ferreira LP. Voz e disfunção temporomandibular em professores. Rev Cefac. 2009, 11(4):630-643.
19. Bianchini EMG. Avaliação fonoaudiológica da motricidade oral - Distúrbios miofuncionais ou situações adaptativas. Rev Dent Press Ortodon Ortopedi Facial. 2001, 6(3):73-83.
20. Tuz HH, Onder EM, Kisnisci RS. Prevalence of otologic complaints in patients with temporomandibular disorder. Am J Ortond Dentofacial Orthop. 2003, 123(6):620-3.
21. Keersmaekers KDDS, De Boever JA, Van Den Berghe L. Otalgia in patients with temporomandibular joint disorders. J Odontol Dent. 1996, 75(1):72-76.
22. Parker WS, Chole RA. Tinnitus, vertigo and temporomandibular disorders. Am J Ortond Dentofacial Orthop. 1995, 107(2):153-8.
23. Felício CM de, Faria TG, Silva MAMR da, Aquino AMCM, Junqueira CA. Desordem Temporomandibular: relações entre sintomas otológicos e orofaciais. Rev Bras Otorrinolaringol. 2004, 70(6):786-793.
24. Mota LAA, Albuquerque KMG, Santos MHP, Travassos RO. Sinais e sintomas associados à otalgia na disfunção temporomandibular. Arq Int Otorrinolaringol. 2007, 11(4):411-415.
25. D'Antonio W E.PA, Ikino CMY, De Castro SM, Balbino APS, Jurado JRP, Bento RF. Distúrbio temporomandibular como causa de otalgia: um estudo clínico. Rev Bras Otorrinolaringol. 2000, 66(1):46-50.
26. Nakashima MMD, Yano HMD, Akita SMD, Tokunaga KMD, Anraku KMD, Tanaka KMD, Hirano AMD. Traumatic Unilateral Temporomandibular Joint Dislocation Overlooked for More Than Two Decades. J Craniofac Surg. 2007, 18(6):1466-1470.
27. Pascoal MIN, Abrão R, Chagas JFS, Pascoal MPBN, Claudiney CC, Magna LA. Prevalência dos sintomas otológicos na desordem temperomandibular: estudo de 126 casos. Rev Bras Otorrinolaringol. 2001, 67(5):627-633.
1 Master. Speech Therapy.
2 Doctor. ENT doctor.
3 Graduation. Speech.
4 PhD. Professor of the Department of Foundations of Speech Pathology at PUC-SP; Coordinator and Teacher of the Specialization Course in Speech -Voz-PUC-SP/COGEAE.
Institution: Catholic University of São Paulo - PUC / SP. São Paulo / SP - Brazil. Mail Address: Ilza Maria Machado - Rua de Barros Napoleon 1058 - Apto.11 - Bairro: Vila Clementino - São Paulo / SP - Brazil - Zip code: 04024-003 - Telephone: (+55 11) 9421-4049 - E-mail: ilzamachado@yahoo.com.br
Article received on March 24th 2010. Article accepted on April 27, 2010.