INTRODUCTIONThe Down Syndrome (DS) or Trisomy 21 is a genetic syndrome characterized by a chromosomal abnormality (extra 21 chromosome). It was initially described in 1866 by Sir John L. H. Down, as the first chromosomal abnormality detected in human kind and may occur in three ways: Free trisomy, translocation or mosaicism (1,2).
Out of the several orthopedic changes found in this syndrome, the Atlantoaxial Instability (AAI) is critical for otorhinolaryngology, and it is represented by a mobility that is higher than the normal of two upper cervical vertebrae C1 and C2 (2). This occurs due to the insufficiency of the transverse ligament, the main stabilizer of the flexo-extension movements between the first and the second cervical vertebra and abnormality of the anatomy of this articulation (3).
The incidence of AAI in patients with DS varies from 10 to 30% (3, 7), it is asymptomatic in most of these individuals and only in 1 to 2% of the cases of AAI diagnosis we found signs and/or symptoms of such change, such as: cervical discomfort, abnormal gait, change to the sphincter control, lesion of the upper motor neuron, paralysis and death (4, 7). About 80% of the symptomatic patients evolve to chronic instability. AAI may be preceded by a cervical trauma, damages caused by sport, orotracheal intubation and head and neck surgery (5). Urgent evaluation and treatment is required for symptomatic patients and regular follow up with the physician associated to the prevention of cervical traumas is crucial for asymptomatic individuals.
The definite diagnosis of cervical spine instability may be difficult. AAI may be detected through the distance between the infero-posterior face of the C1 anterior arc and the anterior process of the odontoid in lateral flexion or extension radiographies, with a limit of up to 4.5 mm (8). The patient with DS who has this measure exceeded will have restrictions for performance of physical activities. However, there may be problems in the AAI radiographic tracking, like: inadequate radiological technique and lack of accuracy to the atlantoaxial distance (6,7).
The objective of this work is to check the prevalence of Atlantoaxial Instability in thirty patients with Down Syndrome who undergo service follow-up in the Clinical Hospital of the UFPR [Federal University of Paraná] and review the need to carry out routine cervical radiography in the patients with prescription to otorhinolaryngologic surgery.
METHODWe performed a prospective study in the population of individuals with Down Syndrome in follow up at the Clinical Hospital of UFPR, in the city of Curitiba, in 2008.
The study was approved by the Ethics Committee in Research of the Clinical Hospital of UFPR.
The parents or persons responsible for the children were duly informed and contacted about the objective of the research and which exam would be made with diagnostic purpose.
30 patients were selected including 13 (43.3%) male and 17 (56.7%) female whose age ranged from 2.5 years to 15 years with a mean age of 9 years old.
Upon authorization of the parents we carried out the application the questionnaire that registered any type of symptomatology presented by the patient: general health state, presence or not of cervical discomfort or torticollis, gait abnormalities, spasticity, paralyses, members weakness, change of sphincter control, previous history of trauma, orotracheal intubation, cervical surgery, recurrent UAI, sports activity. In addition to details of the motor development.
The patients were submitted to radiographic exam of the cervical spine according to the praxis used in the Radiology discipline of the Clinical Hospital and always reported by the same researcher.
The complimentary exam used was the cervical radiography in the anterior, posterior, profile, in flexion and extension for all patients. The radiographic criteria of instability evaluation were based on the measure of the interval between the infero-posterior face of the C1 anterior arc and the odontoid anterior process. We considered it to be normal up to 4.5 mm, between 4.5 and 6 mm suggesting AAI and full AAI over 6 mm at the atlanto-odontoid distance (Figures 1 and 2).
RESULTSAmong the 30 patients with Down Syndrome evaluated through profile, in flexion and extension and antero-posterior cervical spine radiography, we found all with the distance between the infero-posterior face of the anterior C1 arc and the anterior process of odontoid lower than 4.5 mm. Two patients had a distance on the upper limit of normality and were asymptomatic. The average atlanto-odontoid distance in the population studied was of 3.5 mm and there was no case of atlantoaxial instability.
Among the 30 patients submitted to the questionnaire on symptomatology we confirmed that: 2 (6.6%) had cervical discomfort/torticollis, 5 (16.6%) had alterations of the sphincter control (over 4 years of age) and 1 (3.3%) patient complained of pain from the upper and lower ends. All had a delay in the motor development. Repetition airways infection was observed in 50% of the patients.
However, there was no significant association between the signs and symptoms noticed in these patients and the radiological measures.
The results are summarized in Graphic 1.
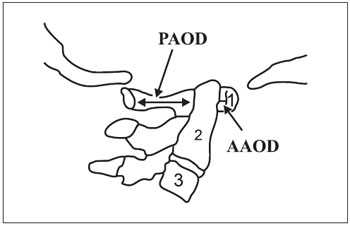
Figure 1. Neutral X-ray.
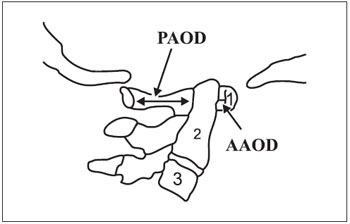
Figure 2. Flexion X-ray.
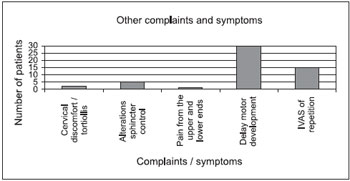
Graphic 1. Complaints and symptoms presented.
Non-traumatic AAI was first described by BERKHEISER and SEIDLER in 1931; and the high frequency of atlantoaxial subluxation (AAS) in patients with DS was described by SPITZER, in 1961.
Since 1983, the Members of the Medical Division of the Special Olympics, have determined that all participants with DS must be evaluated by clinical and radiological exam of the cervical spine so as to research the atlantoaxial instability, and if the atlanto-odontoid distance is over 4.5 mm, such athletes must be left out of sports activities that involve forced flexo-extension movements of the cervical spine, to prevent possible neurological damages due to the medullar compression.
In 1995, the Pediatric American Academy inquired the validity of the AAI radiological triage in DS because, besides the presence of symptomatic instability is rare, the atlantoaxial distance generally regresses or stagnates in time.
MOLIN et al (9) confirmed that out of 36 patients with DS aged between 3 to 41 years old (16 of the male sex and 20 of the female sex), only 5 cases, that is, 13.8% had AAI. Another study, by MINATEL et al (10), with 40 patients with DS, 15% of asymptomatic AAI were diagnosed with radiology while 85% did not present with clinical-radiological evidence without limitation as for the participation in physical education programs and sports activities.
A study carried out in Florianópolis by NAHAS et al (1) researched the incidence of AAI in 17 children with DS aged between 5 and 15 years old and asymptomatic AAI was diagnosed in 2 of them, that is to say, 11.76%. During the work there was a confirmation in some children of neck extension or flexion limitation, apathetic cervical posture, cervical hyperextensibility and reduction of the muscular force and there was no clear association between the signs noticed and the radiological measures.
CROS, LINARES, CASTRO and MANSILLA (11) performed a study with 25 patients with DS that measured the atlanto-odontoid distance (AOD) through radiographies of the cervical spine in flexion and profile followed by computed tomography and tridimensional reconstructions. In 4.3% OAD was verified equal or higher than 5 mm without variation between the measures in flexion and profile. Through this research we conclude that the incidence of AAI has shown quite variable findings of 19 to 30% according to the literature. Therefore, the need for deeper researches on the subject is justified, since in this study the AAI incidence was of 4.3%. Such data are compatible with the findings of this study, in which no atlantoaxial instability was diagnosed in 30 patients with Down Syndrome submitted to cervical spine radiography.
MORTON et al (12), in a 5-year follow-up, did not find the development of AAI in the children studied with admeasurements.
In a prospective study (13), of 1993, the practice of sports was seen not to influence the appearing of neurological changes and exclusion of these patients from sports has no scientific base.
TAYLOR et al (14) concluded the diameter of the medullar canal has a stronger relevance for the AAI evaluation than the atlantoaxial distance, and when the canal is smaller than 13 mm, it suggests a higher risk of medullar lesion. The most adequate complimentary exam to evaluate AAI is Computed Tomography and Magnetic Resonance may be also used. But its use as screening is not frequent due to the need to provide anesthetic induction and its high cost (15, 6).
The AAI research in patients with DS, even asymptomatic ones, is recommended when they had been submitted to intubation for general anesthesia or procedures that involve hyperflexion or hyperextension of the neck or extreme rotation of the head (16).
In fact, the patients with Down Syndrome frequently need upper airways procedures, such as: adenoidectomy and tympanostomy. During these procedures a suitable position of the neck is required for the surgeon to operate, which consists of an important extension of the cervical spine for adenoidectomy and rotation of 90 degrees for tympanostomy. According to the literature review by HARLEY and COLLINS in 1994, it is strongly recommended that all patients submitted to otorhinolaryngologic surgeries be submitted to a preoperative screening to check for AAI, which is justified by the low cost of such screening (17, 18). COHEN, (19), in turn, considers screening not to be cost-effective nor specific or reliable to determine which individuals with AAI have a risk to develop subluxation or spinal compression.
The literature does not provide a consensus as for the actual validity of the radiological triage to research the Atlantoaxial Instability in all patients with Down Syndrome.
However, it suggests that doctors performing risk procedures in patients with Down Syndrome (anesthesia, surgery with cervical manipulation like the otorhinolaryngological procedure) must treat all as susceptible cases and take universal precautions (19).
CONCLUSIONThe Atlantoaxial Instability is a peculiar alteration of the Down Syndrome to which there is no scientific evidences of the need to request radiological routine such as provided by the Medical Division of the Special Olympics.
New studies must be accomplished to define the actual importance of the AAI radiological research in patients with DS and the regular clinical control should always be made in search of the appearing of neurological alterations that form the main trace of medullar compression in the presence of AAI.
BIBLIOGRAPHICAL REFERENCES1. Nahas MV, Rosário AV, Nahas AB, Luza GR. Instabilidade atlanto-axial em crianças com Síndrome de Down na Grande Florianópolis: um estudo piloto. ACM Arq Catarin Méd. 1991, 20(4):149-54.
2. Barros Filho TE, Oliveira RP, Rodrigues NR, Galvão PE, Souza MP. Instabilidade atlanto-axial na Síndrome de Down. Relato de 10 casos tratados cirurgicamente. Rev Bras Ortop. 1998, 33(2):91-4.
3. Siegfried MP. Should Children With Sown Syndrome Be Screened for Atlantoaxial Instability? Arch Pediatr Adolesc Med. 1998, 152:123-125.
4. Ali FE, Al-Bustan AM, Al-Busairi WA, Al-Mulla FA, Esbaita EY. Cervical spine abnormalities associated with Down syndrome. Int Orthopaedics. 2006, 30(4):284-289.
5. Pueschel SM, Scola FH, Tupper TB, Pezzullo JC. Skeletal anomalies of the upper cervical spine in children with Down syndrome. J Pediatr Orthop. 1990, 10(5):607-611.
6. Hata T, Todd, MM. Cervical Spine Considerations when Anesthetizing patients with Down Syndrome. Anesthesiology. 2005, 102(3):680-685.
7. Barros Filho TEP, Oliveira RP, Rodrigues NR, Galvão PE, Souza MP. Instabilidade Atlanto-Axial na Síndrome de Down. Relato de dez casos tratados cirurgicamente. Rev Bras Ortop. 1998, 33(2):91-4.
8. Singer SJ, Rubin IL, Strauss KJ. Atlantoaxial Distance in Patients, Standardization of Measurement. Radiology. 1987, 164:871-872.
9. Molin ED, Molin ECD, Chueire A. Instabilidade de C1-C2 na coluna cervical na Síndrome de Down. Semina. 1988, 9(3):156-8.
10. Minatel E, Ortiz J, Campos RC, Rupp AC. Coluna Cervical na Síndrome de Down. Rev Bras Ortop. 1991, 26(5):131-6.
11. Cros T, Linares R, Castro A, Mansilla F. Estúdio radiológico de lãs alteraciones cervicales em el síndrome de Down. Nuevos hallzgos mediante tomografia computarizada y reconstrucciones tridimensionales. Rev Neurol. 2000, 30(12):1101-7.
12. Morton RE, Khan MA, Murray-Leslie C, Elliott S. Atlantoaxial instability in Down's syndrome: a five year follow up study. Arch Dis Child. 1995, 72(2):115-8; discussion 118-9.
13. Cremers MJ, Bol E, de Roos F, van Gijn J. Risk of sports activities in children with Down's sundrome and atlantoaxial instability. Lancet. 1993, 342(8870):511-4.
14. Taylor TK, Walter WL. Screening of children with Down syndrome for atlantoacial (C1-2) instability: another contentious health question. Med J Aust. 1996, 165(8):448-50.
15. Atlantoaxial instability in Down syndrome: subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics. 1995, 96:151-4.
16. Committee on Sports Medicine: Atlantoaxial instability in Down Syndrome. Pediatrics. 1984, 74(1):152-154.
17. Harley EH, Collins MD. Neurologic sequelae secondary to atlantoaxial instability in Down syndrome. Arch Otolaryngol Head Neck Surg 1994; 120:159-165.
18. Brockmeyer D. Down Syndrome and Craniovertebral Instability. Pediatr Neurosurg. 1999, 31:71-77.
19. Cohen WI. Current dilemmas in Down syndrome clinical care: celiac disease, thyroid disorders, and atlanto-axial instability. Am J Med Genet C Semin Med Genet. Aug 15 2006, 142C(3):141-8.
20. Birrer RB. The Special Olympics athlete: evaluation and clearance for participation. Clin Pediatr (Phila). 2004, 43(9):777-82.
21. Pizzutillo PD, Herman MJ. Cervical spine issues in Down syndrome. J Pediatr Orthop. 2005, 25(2):253-9.
1 Bachelor of Medicine from Faculdade Evangélica do Paraná Resident Doctor of the Otorhinolaryngology Discipline of HC/UFPR.
2 Bachelor of Medicine from UFPR. Resident Doctor of the Otorhinolaryngology Discipline of HC/UFPR.
3 Doctoral Degree in Otorhinolaryngology from Escola Paulista de Medicina (1984). Full Professor of the Federal University of Paraná. President of Pan-American Association of Otorhinolaryngology and Head and Neck and Otorhinolaryngologist - Clinopar
4 Otorhinolaryngologist from SBORL. Otorhinolaryngologist at Hospital Infantil Pequeno Príncipe.
5 Bachelor of Medicine from the Pontifical Catholic University of Paraná. Resident Doctor of the Otorhinolaryngology Service of HC/UFPR.
Institution: Clinical Hospital of the Federal University of Paraná. Curitiba / PR - Brazil. Mail address: Marcos Mocellin - Avenida General Carneiro, 181 - Curitiba / PR - Brazil - Zip code: 80060-900 - Telephone: (+55 41) 3360-1800 - http://www.hc.ufpr.br/Templates/informacoes/fale/fale.html
Article received on August 13, 2010. Approved on October 7, 2010.

