INTRODUCTION Tinnitus is an audiological complaint increasingly considerable in the population that must always be taken as the symptom of some disease or sequela of some aggression undergone by the auditory system. It is characterized by an auditory perception not coming from outside, original from one or both ears, or the head, without a definite location (1, 2).
According to the literature, this symptom affects between 14 and 32% of the population and may be incapacitating in up to 5% of the cases (3).
One of the mostly known classifications for tinnitus is the existence of objective and subjective tinnitus, the first is related to the perception of a sound by the patient and by the examiner and the latter is related to the perception of a sound only by the patient, but the fact that the same alteration may cause both objective and subjective tinnitus limits the clinical application of this classification (4, 5).
Currently the mostly accepted classification for tinnitus takes into account its original source and the anatomophysiology of the auditory system, by dividing it into Auditory tinnitus, that are caused by alterations to the ear, auditory pathways and auditory cortex, and Vascular-Muscular-Auditory tinnitus, by vascular and muscular structures close to the ear and auditory pathways (3).
Tinnitus is a symptom that may be caused by several otological, metabolic, neurological, cardiovascular, pharmacological, odontological and psychological affections and even by a combination of these affections (6, 7).
The hyperacusis is an unproportional growth of the sound intensity sensation that occurs within the auditory pathway, and causes a decrease of the sound tolerance, generally followed by tinnitus. It is characterized by the discomfort with weak or moderate intensity sound, irrespectively of the environment or situation in which it occurs (8).
The prevalence of hyperacusis in the general population is uncertain, but about 25 to 40% of the patients with tinnitus also present with some degree of hyperacusis (9). People with both symptoms feel more uncomfortable with hyperacusis than the tinnitus itself (8).
Another study reported that from each 100 people with otological complaints, 20 are affected by hyperacusis (10).
People with hyperacusis tend to prevent social interactions and situations like listening to music, going to the theater, restaurants and movies, and in severe cases the constant use of ear plugs is frequent (11).
The basic evaluation of hyperacusis is composed by detailed anamnesis connected to Tonal and Vocal Audiometry, Imitanciometry and research of Loudness Discomfort Level - LDL (12), considering the level of discomfort to be hyperacoustic when the results found in two or more frequencies of 250 to 8000 Hz are lower than 90 dB (13).
All efferent fibers original from the most different points of the central nervous system are organized at the level of the Superior Olivary Complex (SOC). From this point, they go down towards the cochlea through two distinct tracts, the Medial Olivary Cochlear Tract, had as the final destiny, the external hair cells (EHC) and the Lateral Olivary Cochlear Tract, responsible for the innervation of the inner hair cells (IHC) (14, 15).
The fibers of the Medial Olivary Cochlear System (MOCS) are originated in the primary auditory cortex, pass through the thalamus and the lower colliculus and arrive at the SOC. From this point, the fibers that originate the MOCS cross the middle line at the level of the IV ventricle floor and get into the cochlea superposed to the lower vestibular nerve fibers through the Oort's vestibulo-cochlear anastomosis (15).
Among the MOCS' functions, there is the auditory figure-bottom ability by which we can concentrate in the sound source and abstain from the bottom noise that, in spite of being an activity of the cortical upper centers, occurs by means of efferent neurons in which the cortex can modulate the afferent message somehow, and the corticothalamic olivary pathway is probably in charge of this selective attention and the cochlear modulation (15- 17).
We remark that through the medial olivary-cochlear tract the MOCS modulates the EHCs and a disorder to this system would be able to generate the mechanisms of tinnitus (15) and hyperacusis (8).
Therefore, due to the participation of the MOCS in the recognition of the auditory stimuli in the presence of competitive noise, the importance of this work is justified aiming to evaluate the speech recognition, in silence and in noise, of normal-hearing individuals and with complaints of tinnitus and hyperacusis, through the test Lists of Sentences in Portuguese (LSP), prepared by COSTA in 1998 (18) and compare the results obtained in both groups.
METHOD This study was performed in the Phonoaudiological Service of the Federal University of Santa Maria (UFSM) and is connected to the research project entitled "Research and Database in Auditory Health", registered in the Office of Projects of the Health Sciences Center of UFSM under no. 019731 and approved in the Ethics Committee in Research under no. 0138.0.243.000-06 in 12/05/2006.
It composes a descriptive, experimental and transversal study in which 19 normal-hearing individuals were evaluated with complaints of tinnitus and hyperacusis, who formed the study group (SG), 11 of the female sex and 8 of the male sex, aged between the range from 21 to 59 years old, and 23 normal hearing individuals without audiological complaints who formed the control group (CG), 13 female and 10 male, between the age range of 19 and 46 years old. All participants, both from the SG and the CG, accepted to take part as volunteers in the study and signed the Free and Informed Consent Term.
Out of which, the results obtained from 29 ears of the SG that presented with tinnitus, hyperacusis and normal hearing in the frequencies of 0.25 to 8 kHz and 46 ears of the CG were considered.
The selection of the individuals was carried out through the media (site, radio and television of the Federal University of Santa Maria and local and regional papers) by means of which information was provided on the study and the relevant audiological symptoms. The persons interested contacted and those who were qualified for the study criteria were scheduled for evaluations.
As an inclusion criterion it was necessary that the SG individuals had complaints of tinnitus and hyperacusis, differently from the CG individuals, who should not present with audiological complaints, and all the individuals from both groups had to have normal hearing in the frequencies from 0.25 to 8 kHz.
Initially all participants were submitted to audiological anamnesis, visual inspection of the external acoustic meatus, threshold and vocal tonal audiometry and acoustic immittance measures, to confirm the presence of normal hearing in the frequencies of 0.25 to 8 kHz in both ears and absence of changes of external and/or middle ear. In the necessary cases, we forwarded for otorhinolaryngological consultation.
For analysis of the tinnitus, the questionnaire Tinnitus Handicap Inventory (THI), prepared by NEWMAN, JACOBSON & SPITZER (19) was applied and adapted to Brazilian Portuguese in 2005 (20). The questionnaire is composed by 25 questions in which the answers are "yes, no, or sometimes" and the marking is of 4, 0 and 2, respectively, and according to the sum, the tinnitus is characterized as degree 1 (0 - 16), slight (only realized in silent places), degree 2 (18 - 36) - light (easily masked by environmental noises and easily forgotten with daily activities), degree 3 (38 - 56) - moderate (realized in the presence of bottom noise, although daily activities may still be done), degree 4 (58 - 76) - severe (almost always realized, takes to disorders of the sleep standards and may interfere with daily activities), and degree 5 (78 - 100) - catastrophic (always realizing disorders in the sleep standards, difficulty to do any activity).
For analysis of hyperacusis, the individuals were submitted to LDL in the frequencies of 0.25 to 8 kHz in both ears that, as proposed by GOLDSTEIN e SHULMAN (13), is classified in negative degree (threshold of discomfort 95 dB or more in all frequencies), light (threshold of discomfort 80-90 dB in two or more frequencies), moderate (threshold of discomfort 65-75 dB in two or more frequencies), and severe (threshold of discomfort 60 dB or less in two or more frequencies).
All individuals taking part in the study, both in the SG and the CG, were submitted to the LSP to determine the Sentences Recognition Threshold in Silence (LRSS) and the Sentences Recognition Threshold in Noise (LRSR). The latter is expressed through the Signal-Noise ratio (S/N) that is the difference between the average intensity of presentation of sentences less the noise, fixed at 65 dB NA.
The test is composed by a list of 25 sentences called 1A (21), other seven lists, each with 10 phonetically balanced sentences, all with simple structure and period and extension ranging from four to seven words, which were called 1B, 2B, 3B, 4B, 5B, 6B and 7B (22, 23) and a noise with spectrum of speech (24). Finally, COSTA (18) gathered in a book and CD the material developed in these studies, by presenting LSP test application results and strategies, in addition to bringing the sentences (1A and 1B to 7B) and the noise with the same spectrum of speech, reproduced in CD and recorded from the original matrix.
The measures were obtained in acoustically treated cabin, by using Fonix brand two-channel audiometer, model FA-12, and TDH 39 ear plugs. The sentences were presented through a Compact Disc Player Digital Toshiba, model 4149, coupled to the audiometer.
In the LSP application, a training was initially held through the presentation of the 1A list sentences, both in silence and in the presence of competitive noise, so that the individuals got used to the evaluation. For obtaining LRSS and LRSR, the initial intensity of stimulus presentation was of about 5 dB above the required for each individual to obtain a hit in the recognition of the first sentence based on the training carried out previously.
The stimulus presentation interval was of dB NA up to the first change in the response pattern and later the intervals changed from 2.5 dB NA between each other to the end of the list. Moreover, in the LRSR research the noise was maintained constantly at 65 dB NA.
As noticed by the author of the material, through the spectrographic analysis and based on the researches results, the existence of a difference of 7 dB between speech and noise, a procedure was adopted for the calculation of the LRSS and LRSR, a subtraction of 7 dB from the average speech values presented and registered, according to the observation on the equipment's dial.
The technique used for presentation of the sentences was based on the ascending-descending sequential or adaptive strategy, described by LEVITT and RABINNER (25), which allowed us to determine the speech recognition threshold, level required for the individual to identify properly, about 50% of the stimuli presented.
After performance of the procedures the individuals were given guidelines on the evaluations carried out and the relevant audiological symptoms.
The statistical analysis was carried out through the program Stata 10.0 - Statistics / Data Analysis. To review the variable behavior, we used the normality test Skewness and kurtosis test. After confirming the normal distribution of data, the performance of the CG and SG individuals was compared by using the Student T-test. To correlate the SG individuals' performance according to the degree of the audiological symptoms, the Pearson's Correlation test was applied. The p<0.05 was deemed to be a significant result with reliability interval of 95%.
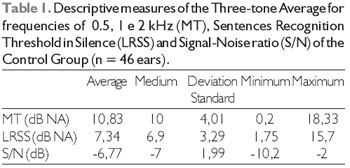
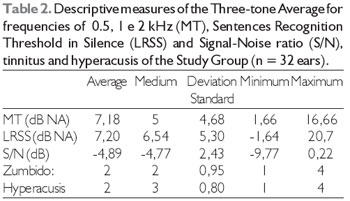
RESULTSIn Tables 1 and 2 the descriptive analysis of the results of variables considered in the Control Group and the Study Group will be described, respectively, by remarking that all variables of both groups have followed a normal distribution.
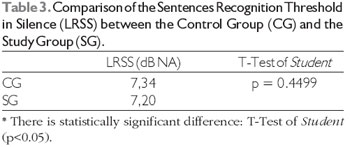
By comparing the performance on the speech recognition in silence, among the normal hearing individuals with and without tinnitus and hyperacusis audiological complaints, we noticed the participants of both groups had a similar performance in this communication scenario, as described in Table 3.
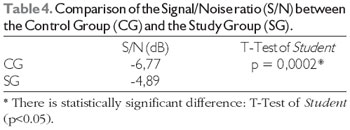
In the situation of speech recognition in noise, we observed a lower performance of the SG when compared with the CG, including statistically significant difference (p<0.05) - Table 4.
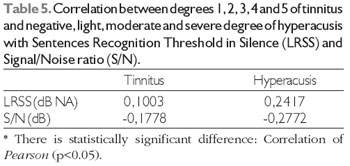
When comparing degrees 1, 2, 3, 4 and 5 of tinnitus and the negative, light, moderate and severe degrees of hyperacusis, the performance of the SG individuals in the speech recognition in silence and in noise, we did not verify any correlation between the different degrees of the audiological symptoms and the speech recognition, both in silence and in noise - Table 5.
DISCUSSIONThe results obtained from the evaluation carried out show that the speech recognition in silence is similar in the normal hearing individuals without audiological complaints of tinnitus and hyperacusis, the LRSS obtained for the CG was of 7.34 dB NA and for the SG of 7.20 dB NA.
The fact that the SG normal hearing individuals with audiological complaints behaved in the same manner in silence as the CG normal hearing individuals without audiological complaints, confirms the capacity for speech recognition in silence is bound to the tonal thresholds.
Prior studies have already confirmed such relationship between the audibility itself and the speech recognition in silence as previously performed (26) in which 240 young adults were evaluated in silence and obtained an LRSS in 6.2 dB NA, compatible with the average of the three-tone thresholds, 7.22 dB NA in the frequencies of 0.5, 1 and 2 kHz.
This correlation between the audibility thresholds and LRSS was also confirmed by another study (27), in which the average LRSS obtained in 200 ears examined was 6.15 dB NA and the average of tonal thresholds for the frequencies of 0.5, 1 and 2 kHz, 8.55 dB NA, and the statistical analysis confirmed a significant correlation between them.
By reviewing the three-tone averages and the LRSS of the individuals in this study, we noticed in the CG the tonal threshold average for frequencies of 0.5, 1 and 2 kHz was of 10.83 dB NA and the LRSS, 7.34 dB NA, with better values for the LRSS. The same was found in studies carried out previously, in which the authors stated this is expected, since the sentences provide acoustic and linguistic clues with meaning (26, 27).
By taking into account the same variables in the SG, we notice it is not the case, and the average of the tonal thresholds for frequencies 0.5, 1 and 2 kHz in 7.18 dB NA and the LRSS, 7.20 dB NA is quite similar. This may be related to the difficulty for the individuals to draw their attention from their tinnitus, with specific frequency and intensity, and be attentive to the acoustic information.
As for the unfavorable communication scenario, in the presence of competitive noise, we noticed the CG had an average S/N ratio of -6.77 dB, minimum S/N ratio of -2 dB and maximum ratio of -10.2, and the SG had an average S/N ratio of -4.89 dB, minimum of 0.22 dB and maximum of -9.77 dB, respectively, by confirming that despite all of them are normal-hearing individuals, the performance in this situation was different, and the SG obtained a lower performance when compared to the CG, with a statistically significant difference for the mean S/N ratio, and the minimum value for the S/N ratio of the SG was positive.
It's worth emphasizing that when it comes to the S/N ratio, the higher the negative number, the more unfavorable it will be and the better the performance of the subjects upon the competitive noise will be too.
Considering in this context the participation of the MOCS in the recognition of auditory stimuli in the presence of competitive noise (15 - 17), and that a disorder in this system is connected to the mechanisms of tinnitus (15) and hyperacusis (8), the normal hearing individuals who have complaints of tinnitus and hyperacusis may have a damage in such communication situations due to a change to the functioning of the efferent fibers of MOCS to keep the selective attention and a suitable cochlear modulation.
Moreover, we standout that when it comes to the recognition of the speech in noise, slight variations in the S/N ratio may provoke large changes to the capacity to recognize the speech. Some studies state that at each 1 dB of change to the S/N ratio, the speech understanding may be changed in 12% (28), 13.2% (29) and 18% (30).
Therefore, by making a scheme based on the study described above (28), also accomplished through the LSP (18), the difference in the S/N ratio confirmed between the SG and the CG of 1.88 dB may indicate a damage of about 22.56% for normal hearing individuals with complaints of tinnitus and hyperacusis to recognize the speech in the presence of competitive noise.
Other results regarding the performance in the recognition of speech in the presence of competitive noise of young normal hearing adults, obtained through the same evaluation instrument were described by other authors who have found an average S/N ratio of -5.29 dB from the evaluation of 240 individual (26), mean S/N ratios of -6.34 dB (31), -8.02 dB NA in the right ear and -7.41 dB NA in the left ear (32) and -6.31 dB NA in the right ear and -6.68 dB NA in the left ear (33).
By reviewing and comparing the findings mentioned above, with those from the CG, -6.77 dB, we verified that these are close to them, and even better than those found in a prior study (26), -5.29 dB, that proposed to set up normality values evaluating a higher number of participants. However, the SG was below such values, -4.89 dB, as well as all other mentioned researches, which reinforces the higher difficulty of such normal hearing individuals with complaints of tinnitus and hyperacusis to recognize the speech in noise.
When the intergroup performance of the normal hearing individuals with complaint of tinnitus and hyperacusis is analyzed as for speech recognition in silence and noise, no correlation was confirmed between the different degrees of the audiological symptoms, tinnitus and hyperacusis, both with LRSS and S/N ratio.
The fact the degree of tinnitus and hyperacusis is determined based on subjective measures, the THI and LDL questionnaire, in which the individual regards with which frequency the symptom interferes with the specified situation and the uncomfortable intensity for the frequencies of 0.25 to 8 kHz, respectively, may make the precise measurement of the variables bound to the degree of the relevant symptoms difficult and thus influence the correlation with the performance in speech recognition in silence and noise.
CONCLUSIONThe findings of this study indicate the normal hearing individuals with or without audiological complaints of tinnitus and hyperacusis had a similar performance in the speech recognition in silence.
The results indicate that it was not noticed when the speech recognition is evaluated in the presence of competitive noise, and the normal hearing individuals with tinnitus and hyperacusis had a lower level performance in this communication scenario when compared to the normal hearing individuals, with rather statistically significant difference.
We also confirmed the different degrees of the audiological symptoms of normal hearing individuals and complaints of tinnitus and hyperacusis do not interfere with the performance to recognize the speech, both in silence and in noise.
Based on the probable influence the presence of tinnitus and hyperacusis have on the speech recognition in noise it would be critical that measures evaluating the auditory capacities were presented as a compliment of routine audiological evaluation in case of patients with such complaints, even in the absence of the audibility involvement.
Moreover, we standout the discomfort of the individual that mentions such complaints and the reflex on the life quality, from a clinical viewpoint, since the symptoms are a consequence of some change to the auditory system and/or in other organs, the operation of a multidisciplinary staff may be valid, which involves psychiatrists or psychologists, neurologists, endocrinologists, cardiologists, dentists and physiotherapists, in addition of the otorhinolaryngologist and phonoaudiologist aiming to the investigation and possible treatments.
Therefore, there is the possibility to dimension the consequences of such complaints in the patient's communication and intervene in a personalized manner in the possible causes and impacts of each case in an attempt to mitigate the audiological complaints and improve the quality of life and welfare of the individual.
BIBLIOGRAPHICAL REFERENCES1. Meyer B et al. Définitions et Classifications. In: Meyer B, editor. Acouphènes et Hyperacousie. Paris: Société Française dOto-rhino-laryngologie et de Chirurgie de la Face et du Cou; 2001, p. 3-8.
2. Sanchez TG, Ferrari GMS. O que é zumbido? In: Samelli AG. Zumbido: avaliação, diagnóstico e reabilitação: abordagens atuais. São Paulo: Lovise; 2004, pp.17-22.
3. Azevedo AA, Figueiredo RR. Atualização em Zumbido. Rev Bras Otorrinolaringol. 2004, 70(1):27-40.
4. Sanchez TG, Netto BM, Sasaki F, Santoro PP, Bento RF. Zumbidos gerados por alterações vasculares e musculares. Arq Fund Otorrinolaringol. 2000, 4(4):136-42.
5. Person OC. Avaliação dos potenciais evocados auditivos de tronco cerebral em portadores de indivíduos com tinnitus antes e após tratamento com administração sistêmica de compostos com zinco. Ribeirão Preto, 2003, p. 125, (Tese de mestrado - Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo).
6. Sanchez TG. Reabilitação do paciente com zumbido. In: Campos CA, Costa HO. Tratado de Otorrinolaringologia. São Paulo: Roca; 2002, Vol. 2, pp. 311-24.
7. Sanchez TG. Zumbido: Análise crítica de uma experiência de pesquisa. São Paulo, 2003, (Tese de Livre-Docência, Faculdade de Medicina da Universidade de São Paulo).
8. Jastreboff PJ, Jastreboff MM. Tinnitus Retrainning Therapy (TRT) as a method of tinnitus and hiperacusis patients. J Am Acad Audiol. 2000, 11(3):162-77.
9. Jastreboff, PJ, Hazell, JWP. A neurophysiological model for tinnitus: clinical implications. Br J Audiol. 1993, 27:7-17.
10. Magalhães SL, Fukuda Y, Liriano RI, Chami FA, Barros F, Diniz FL. Relation oh hyperacusis in sensoneural tinnitus patients with normal audiological assessment. Int Tinnitus J. 2003, 9(2):79-83.
11. Valente M, Goebel J, Duddy D, Sinks B, Peterein J. Evaluation andtreatment of severe hyperacusis. J Am Acad Audiol. 2000, 11(6):295-9.
12. Knobel KAB, Sanchez TG. Atuação dos fonoaudiólogos do estado de São Paulo (Brasil) na avaliação de pacientes com queixa de zumbido e/ou hipersensibilidade a sons. Pró-Fono. 2002, 14(2):215-24.
13. Goldstein B, Shulman A. Tinnitus - Hyperacusis and the Loudness Discomfort Level Test - A Preliminary Report. Int Tinnitus J. 1996, 2:83-9.
14. Warr WB. Efferent components of the auditory system. Ann Otol Rhinol Laryngol. 1980, 89:114-20.
15. Breuel MLF, Sanchez TG, Bento RF. Vias Auditivas Eferentes e seu Papel no Sistema Auditivo. Arq Int Otorrinolaringol. 2001, 5(2):149.
16. Giraud AL, Garnier S, Micheyl C, Lina G, Chays A, Chéry-Croze S. Auditory efferents involved in speech-in-noise intelligibility. Neuroreport. 1997, 8(7): 1799-83.
17. Grataloup C, Hoen M, Veuillet E, Collet L, Pellegrino F, Meunier F. Speech Restoration: An Interactive Process. J Speech Lang Hear Res. 2009, 52 (4):827-38.
18. Costa MJ. Listas de sentenças em português: apresentação e estratégias de aplicação na audiologia. Santa Maria: Pallotti, 1998.
19. Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1996, 122(2):143-8.
20. Ferreira PEA, Cunha F, Onishi ET, Branco-Barreiro FCA, Ganança FF. Tinnitus Handicap Inventory: adaptação cultural para o português. Pró-Fono. 2005, 3(17):303-10.
21. Costa MJ, Iório MCM, Mangabeira-Albernaz PL. Reconhecimento de fala: desenvolvimento de uma lista de sentenças em português. Acta Awho. 1997, 16(4):164-73.
22. Costa M. J. Desenvolvimento de listas de sentenças em português. São Paulo, 1997, p. 102, (Tese de doutorado - Universidade Federal de São Paulo/Escola Paulista de Medicina).
23. Costa MJ, Iório MCM, Albernaz PLM. Desenvolvimento de um teste de fala para avaliar a habilidade de reconhecer a fala no silêncio e no ruído. Pró-fono. 2000, 12(2):9-16.
24. Costa MJ, Iorio MCM, Albernaz PLM, Cabral Junior EF, Magni AB. Desenvolvimento de um ruído com espectro de fala. Acta Awho. 1998, 17(2): 84-9.
25. Levitt H, Rabiner LR. Use of a sequencial strategy in intelligibility testing. J Acoust Soc Am.1967, 42(3):609-12.
26. Costa MJ, Daniel RC, Santos SN. Reconhecimento de sentenças no silêncio e no ruído em fones auriculares: valores de referência de normalidade. Revista CEFAC. 2010. NO PRELO.
27. Soncini F, Costa MJ, Oliveira TMT, Lopes LFD. Correlação entre limiares de reconhecimento de sentenças no silêncio e limiares tonais. Rev Bras Otorrinolaringol. 2003, 69(5):672-7.
28. Henriques MO, Costa MJ. Índices percentuais de reconhecimento de sentenças em campo livre de indivíduos adultos In: 22º Encontro Internacional de Audiologia, 2007, Natal. Anais do 22º Encontro Internacional de Audiologia. Meio digital, 2007.
29. Wagener K C. Factors influencing sentence intelligibility in noise. Göttingen, 2003, p. 131 (Dissertação de mestrado - Göttingen University).
30. Smoorenburg GF. Speech reception in quiet and in noisy conditions by individuals with noise - induced hearing loss in relation to their tone audiogram. J Acoust Soc Am. 1992, 91(1):421-37.
31. Cóser PL, Costa MJ, Cóser MJ, Fukuda Y. Reconhecimento de sentenças no silêncio e no ruído em portadores de perda auditiva induzida pelo ruído. Rev Bras Otorrinolaringol. 2000, 66(4):362-70.
32. Soncini F, Costa MJ, Oliveira TMT. Queixa de Dificuldade para Reconhecer a Fala x Limiares de Reconhecimento de Sentenças no Ruído em Normo-Ouvintes com Mais de 50 Anos. Fono Atual. 2003, 6(26):4-11.
33. Freitas CD, Lopes LFD, Costa MJ. Confiabilidade dos limiares de reconhecimento de sentenças no silêncio e no ruído. Rev Bras Otorrinolaringol. 2005, 71(5):624-32.
1 Phonoaudiologist.
2 Doctoral Degree in Sciences of Human Communication Disorders from the Federal University of São Paulo. Assistant Professor of the Phonoaudiology Department of the Federal University of Santa Maria.
Institution: Universidade Federal de Santa Maria - USFM. Porto Alegre / RS - Brazil. Mail address: Tais Regina Hennig - Rua Marechal Floriano Peixoto, 1408 - Apto. 302 - Bairro: Centro - Santa Maria / RS - Brazil - Zip code: 97015-372 - Telephone: (+55 55) 9162-3343 - E-mail: tha.hennig@gmail.com
Article received on August 23, 2010. Approved on October 1st, 2010.