INTRODUCTIONGranulomatoses are systemic diseases integrating the differentiated diagnosis of numerous affections of the respiratory tract, on one hand due to the preference for this system, on the other hand for the polymorphism of their clinical manifestations. In this group, there are sarcoidosis, chronic inflammatory disease of undetermined etiology, which, in most cases, impairs the lungs, visceral and parietal pleura, hilar and mediastinal lymph nodes. In the head and neck area, they can cause lymphadenopathy, facial palsy, parotid swelling, eye, and nose and larynx lesions, however rare in a separate way.
Laryngeal sarcoidosis is an underdiagnosed disease, whether for lack of specific detecting tests, turning the diagnosis into an exclusion one, or for the diversity of criteria to be analyzed, so that the diagnostic suspicion can be confirmed (1). The clinical features vary from the asymptomatic form to severe cases, mainly when there is an obstruction of the airways. Differences in the characteristics of the disease are observed according to age, and a lower frequency of the isolated laryngeal impairment and a more evident symptomatology are seen during the pediatric age group.
New technologies have been used for a diagnosis, such as PET/CT (positron-emission tomography), widely used in malign neoplasias, but since it is not a specific tumor exam, it can be used to detect benign conditions like sarcoidosis.
The objective of this review is to update the sarcoidosis data, from etiology to treatment, by emphasizing the laryngeal impairment scarcely described in literature and approaching an exhaustive investigation in its differentiated diagnosis.
METHODThis review was performed by searching subject describers 'sarcoidosis', 'laryngeal diseases' and 'larynx' on Medline, Lilacs and Scielo databases, including English and Portuguese articles published between 1973 and 2008. From the primary selection, new relevant scientific works found in the references were added.
LITERATURE REVIEWEpidemiologySarcoidosis happens to people at all ages, sexes and races, however there are some differences in the characteristics and frequency for likely genetic and environmental factors involved. Typically, it occurs in young adults aged between 20 and 40, and it is discreetly prevalent in women. In the USA, a higher prevalence was identified in the black (35.5/100,000 inhabitants) compared with the white population (10.9/100,000). As to the African continent, it is noticed there is a higher prevalence in the black, however at lower ratios. In the Scandinavian countries, the highest prevalence is found around 64/100,000 in Sweden and 26.7/100,000 in Norway (2). In Brazil, the prevalence in the general population was estimated around 10/100,000 inhabitants (3). The laryngeal involvement occurs in around 0.5-8.3% of the patients, and its isolated presence in this organ is still scarcer.
EtiologyA number of etiologic factors have been associated with likely causes of sarcoidosis, considering the possibility that environmental infectious or non-infectious agents do not unleash a series of immunological and inflammatory events, with a final transformation of macrophages into giant cells and epithelioids composing granuloma blocks and characterizing the disease in genetically susceptible people (6, 7).
Sarcoidosis usually occurs in individuals exposed to environments in which other granulomatoses are proven to occur, particularly, occupational exposure to insecticides, agricultural jobs, bird raising and humid and musty places, typically associated with the exposture to bioaerosol (8).
The genetic susceptibility is demonstrated by the evidence of a higher prevalence in the family and a correlation of some genotypes with the severity and chronic feature of the disease (9, 10), as well as the demonstration of the association with some HLA alleles (DRB1 and DQB1), (11, 12).
Due to the similarity of the clinical and histological features with diseases caused by fungi and microbacteria, the likelihood of transmission in transplanted patients, an increase in antibodies and the detection in tissues of some agents like Propionibacter acnes suggests an infectious case for sarcoidosis (13, 14).
Clinical ManifestationsThree clinical standards are identified in patients diagnosed of sarcoidosis: without symptoms, unspecific constitutional symptoms and organ-specific symptoms (1). The asymptomatic patients have an investigation starting from alterations found in the routine thoracic x-ray and are around 30-50% of the total (15, 16). The symptomatic patients show unspecific complaints such as fatigue, fever and loss of weight; or associated with organ-specific symptoms. Regarding larynx, the most common signals and symptoms are pharyngeal globe, dyspnea, dysphonia, dysphagia and dry cough. Most severe cases can evolve with a stridor and an obstruction of the airway, sometimes requiring a tracheotomy (11, 17).
Laryngeal sarcoidosis patients do not necessarily show the systemic form: in BENJAMIN et al's review (18), out of five patients with laryngeal lesions, only one showed a generalized disease; in NEEL AND MCDONALD's reports (4), out of thirteen patients having laryngeal lesions, seven showed an impairment of other organs.
The laryngoscopy findings are shown as edematous, elevated and pale mucosa, in the following sites in a decreasing frequency order: Epiglottis, arytenoid, aryepiglottic folds and vestibular folds (19). This major impairment of the supraglottis probably occurs due to the big amount of lymphatic vases in this area, which are stretchered by replacing the architecture by sarcoid deposits or subcutaneous foci of the disease (Figure 1) (20). More rarely, it can involve subglottis and in 24% of the cases, vocal folds, also causing their immobility, whether for an impairment of the vagum nerve or their fixation by sarcoid infiltration in the crycoaritenoid joint, a diagnosis sometimes hard to be made by electromyography (21,22).
Pediatric Sarcoidosis This is an uncommon disease in the pediatric age group, having an approximate 1.02/100,000 ratio (23). It is usually shown more symptomatically than in adults, probably because the disease is more detected in asymptomatic adults by a routine thoracic x-ray, what is not usually performed in children (24). The most common symptoms are lethargy and fatigue, but cough, fever and loss weight are also frequent (25).
Its extrapulmonary characteristic is more frequent than in adults; however the isolated laryngeal impairment is more infrequent as related by KENNY et al. (26). The laryngeal involvement happens in both the pre-pubertal and in the post-pubertal age group and dyspnea, cough and hoarseness are frequent (27).
DiagnosisFor a sarcoidosis diagnosis, 3 criteria must be met: compatible clinical-radiological findings, histological sample represented by non-necrotizing granulomas and exclusion of other granulomatoses or diseases having similar findings.
The thoracic x-ray images usually show a hilar lymphadenopathy and a pulmonary infiltrate (6). The larynx images are more unspecific, among which are sideface cervical X-ray, what can show an increase in epiglottis similar to "the thumb sign" of the acute epiglottis, or the computed tomography showing a dense mass of soft parts in the impaired topography, usually supraglottis (18,28).
Another exam that has been mostly recently used is FDG PET (positron emission tomography), which has identified an increase in detecting fluoro-deoxy-glycolysis not only in malign lesions but in granulomatous lesions with sarcoidosis (29, 30).
BRAUN et al. (31) demonstrated an 85% sensitivity of PET/CT to detect active sites of laryngeal-pharyngeal sarcoidosis proven by a biopsy. Additionally, it can be a useful method to warn about the presence of the laryngeal involvement in patients with a previous history of sarcoidosis without typical symptoms (29).
Evidence of laryngeal lesion associated with the histological sample of another site (e.g., lung) compatible with sarcoidosis are not sufficient to determine a laryngeal impairment by sarcoidosis, because in literature cases of pulmonary sarcoidosis associated with a laryngeal carcinoma are described (32). Therefore, in order to reach a diagnosis of laryngeal sarcoidosis, a biopsy of the lesion in this topography must be performed, and the result is shown as non-necrotizing epithelioid granuloma (1, 3, 2).
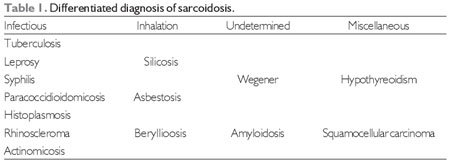
In order to exclude other diseases integrating the differentiated diagnosis, a survey of alcohol-acid-resistant fungi and bacillus, as well as a culture for bacteria and fungi from the biopsied specimen; survey of syphilis (VDRL), Wegner's granulomatous (cANCA), tuberculkosis (PPD) and a serology for histoplasmosis and paracoccidioidomicosis (1,18).
Differentiated DiagnosisSince sarcoidosis is an exclusion diagnosis (1, 21), all the supplementary methods must be used to investigate diseases having similar manifestations in the clinical, radiological and, especially, histological features (Table 1).
TreatmentThe clinical course of sarcoidosis is very diversified: 60-70% of patients showing a spontaneous remission, 10-20% showing permanent sequels and the mortality is 1-5% usually for pulmonary, cardiological and neurological complications (1). The treatment of choice is systemic corticotherapy; usually the drug used is prednisone at a dose of 40-60 mg/day in adults and mug/kg/day in children, for a total period of 6-12 months (34, 35). In the immune cases or with an intention of reducing the side effects of corticoids, cytotoxic agents, such as methotrexate and azathioprine, can be used effectively, and only in resistant cases, more toxic drugs, such as cyclophosphamide and chlorambucil can be used (36,37).
When there is no satisfactory improvement of laryngeal lesions with a systemic treatment and the patient appears to be symptomatic, an option is an intraregional corticoid injection (triamcinolone or methylprednisolone), which will reach high local concentrations with reduced side effects (26). The results are diverse, but in some cases of airway obstructions, decannulation of tracheostomy is achieved by this therapy (27). When there is an imminent of respiratory insufficiency for a high obstructon, tracheostomy must be performed beforehand and, if there is no response, injectable corticotherapy is chosen for resection of obstructive lesions, in most cases, partial resection of epiglottis through CO2 laser or cold instruments (26). A radiotherapy treatment is also described for these lesions with the disadvantage of a likely local carcinogenic effect (38).

Figure 1. Laryngeal sarcoidosis - Image provided by Dr. Enric Massana.
In this review, the breakthroughs in the diagnosis and treatment of sarcoidosis are shown; however it is a disease that remains without a clear etiology and physiopathology, becoming an exclusion diagnosis due to both the lack of precise exams and its likely multifactor background. Laryngeal impairment, however infrequent, is a suspicion mainly when there is a precedent history of systemic sarcoidosis, and the research for differentiated diagnosis must be wide-ranging so as to prevent severe diseases like malign neoplasia from being unnoticed.
REFERENCES1. Schwartzbauer HR, Tami TA. Ear, nose and throat manifestations of sarcoidosis. Otolaryngol Clin N Am. 2003, 36:673-84.
2. James DG, Hosoda Y. Epidemiology in sarcoidosis and other granulomatous disorders. New York: Marcel Dekker; 1994. (Lung biology in health and disease).
3. Bethlem NM. Epidemiology of sarcoidosis in Brazil. Sarcoidosis. 1985, 2:162.
4. Neel HB III, McDonald TJ. Laryngeal sarcoidosis: report of 13 patients. Ann Otol Rhinol Laryngol. 1982, 91(4 Pt 1):359-62.
5. Fortune S, Courey MS. Isolated laryngeal sarcoidosis. Otolaryngol Head Neck Surgery. 1998, 118(6):868-70.
6. Weinberger SE. Sarcoidosis. In: Goldman: Cecil medicine. Philadelphia: Elsevier Saunders; 2007. chapter 95.
7. Shigehara K, Shijubo N, Ohmichi M, et al. Enhanced mRNA expression of Th1 cytokines and IL-12 in active pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2000, 17(2):151-7.
8. Newman LS, Rose CS, Bresnitz EA, Rossman MD, Barnard J, Frederick M, et al. A case control etiologic study of sarcoidosis: environmental and occupational risk factors. Am J Respir Crit Care Med. 2004, 170:1324-1330.
9. Brennan NJ, Crean P, Long JP, et al. High prevalence of familial sarcoidosis in an Irish population. Thorax. 1984, 39(1):14-8.
10. Abe S, Yamaguchi E, Makimura S, et al. Association of HLA-DR with sarcoidosis. Correlation with clinical course. Chest. 1987, 92(3):488-90.
11. Rossman MD, Thompson B, Frederick M, et al. HLA-DRB1 1101: a significant risk factor for sarcoidosis in blacks and whites. Am J Hum Genet. 2003, 73:720-35.
12. Iannuzzi MC, Maliarik MJ, Poisson LM, Rybicki BA. Sarcoidosis susceptibility and resistance HLA-DQB1 alleles in African Americans. Am J Respir Crit Care Med. 2003, 167:1225-31.
13. Heyll A, Meckenstock G, Aul C, et al. Possible transmission of sarcoidosis via allogeneic bone marrow transplantation. Bone Marrow Transplant. 1994, 14(1):161-4.
14. Moller DR, Chen ES. What causes sarcoidosis? Current Opinion in Pulmonary Medicine. 2002, 8:429-434.
15. Siltzbach LE, James DG, Neville E, et al. Course and prognosis of sarcoidosis around the world. Am J Med. 1974, 57(6):847-52.
16. Winterbauer RH, Belic N, Moores KD. Clinical interpretation of bilateral hilar adenopathy. Ann Intern Med. 1973, 78(1):65-71.
17. Vaz FM, Samuel D. Postcricoid sarcoid mimicking a malignancy: A lesson to remember. Otolaryngol Head Neck Surg. 2000, 123:150.
18. Benjamin B, Dalton C, Croxson G. Laryngoscopic Diagnosis Of Laryngeal Sarcoid. Ann Otol Rhinol Laryngol. 1995, 104:529-31.
19. Dean CM, Sataloff RT, Hawkshaw MJ, Pribikin E. Laryngeal sarcoidosis. J Voice. 2002, 16(2):283-8.
20. Hernández PE, Casas AA, Massana EF, et al. Sarcoidosis Laríngea Aislada. Acta Otorrinolaringol Esp. 2003, 54:117-20.
21. Caporrino Neto J, Cervantes O, Jotz GP, Abrahão M. Doenças granulomatosas da Laringe. Acta Awho. 1998, 17(1):6-10.
22. Bower JS, Belen JE, Weg JG, Dantzer DR. Manifestations and treatment of laryngeal sarcoidosis. Am Rev Respir Dis. 1980, 122:325-32.
23. Hoffmann AL, Milman N, Byg KE. Childhood sarcoidosis in Denmark 1979-1994: incidence, clinical features and laboratory results at presentation in 48 children. Acta Paediatr. 2004, 93:30-6.
24. Kendig EL. The clinical picture of sarcoidosis in children. Pediatrics. 1974, 54: 289-92.
25. Kendig EL, Brummer DL. The prognosis of sarcoidosis in children. Chest. 1976, 70:351-353.
26. Kenny TJ, Werkhaven J, Netterville JL. Sarcoidosis of the Pediatric Larynx. Arch Otolaryngol Head Neck Surg. 2000, 126:536-39.
27. Rybak L, Falconeer R. Pediatric Laryngeal Sarcoidosis. Ann Otol Rhinol Laryngol. 1987, 96:670-73.
28. Palacios E, Smith A, Gupta N. Laryngeal sarcoidosis. Ear, Nose and Throat Journal. 2008, 252-53.
29. Kaira K, Ishizuka T, Yanagitani N, Sunaga N, Hisada T, Mori M. Laryngeal Sarcoidosis Detected by FDG Positron Emission Tomography. Clin Nucl Med. 2008, 33:878-79.
30. Avram AM, Mackie GC, Schneider BJ, et al. Differentiation between carcinoid and sarcoid with F-18 FDG PET and In-111 pentetreotide. Clin Nucl Med. 2006, 31:197-200.
31. Braun JJ, Imperiale A, Schultz P, Molard A, Charpiot A, Gentine A. Pharyngolaryngeal sarcoidosis: Report of 12 cases. Otolaryngology-Head and Neck Surgery. 2008, 139:463-65.
32. Gal AA, Koss MN. The pathology of sarcoidosis. Current Opinion in Pulmonary Medicine. 2002, 8:445-451.
33. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007, 357:2153-65.
34. Martinez JAB. Doenças intersticiais pulmonares. Medicina. 1998, 31:247-256.
35. Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med. 1997, 336(17):1224-1234.
36. Baughman RP, Lower EE. A clinical approach to the use of methotrexate for sarcoidosis. Thorax. 1999, 54(8):742-6.
37. Lewis SJ, Ainslie GM, Bateman ED. Efficacy of azathioprine as second-line treatment in pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 1999, 16(1):87-92.
38. Carasso B. Sarcoidosis of the larynx causing airway obstruction. Chest. 1974, 65(6):693-5.
1) Otorhinolaryngologist. Taking Master Degree at the Federal University of São Paulo's Department of Otorhinolaryngology and Head and Neck Surgery (UNIFESP-EPM).
2) Otorhinolaryngologist. Taking Doctorate Degree at the Federal University of São Paulo's Department of Otorhinolaryngology and Head and Neck Surgery (UNIFESP-EPM).
3) Otorhinolaryngologist. Professor Doctor at the Federal University of São Paulo's Department of Otorhinolaryngology and Head and Neck Surgery (UNIFESP-EPM).
4) Otorhinolaryngologist. Assistant Professor at the Federal University of São Paulo's Department of Otorhinolaryngology and Head and Neck Surgery (UNIFESP-EPM).
5) Doctor. Taking Specialization Degree in Otorhinolaryngology at the Federal University of São Paulo (UNIFESP-EPM).
Institution: Department of Laryngology and Voice in Otorhinolaryngology at the Federal University of São Paulo - Paulista School of Medicina (UNIFESP-EPM). São Paulo / SP - Brazil. Mailing address: Bruno Teixeira de Moraes Rua Pedro de Toledo, 957 - Vila Clementino - São Paulo/SP - Brazil - ZIP Code: 04039-032 - Telephone: (+55 11) 5573-2740 - Email: moraesbruno.orl@hotmail.com
Article received on January 23, 2010. Article approved on April 24, 2010.