INTRODUCTIONChoanal polyps are types of solitary, benign tumors, which come from one paranasal sinus and pass over drainage ostium of this sinus projecting itself to the choana up to nasal-pharynx. They present an intrasinusal portion, an ostial one, and another extrasinusal (1). They can come from maxillary sinus, sphenoid and ethmoid (1,2), being questioned in relation to its formation from frontal sinus (3,4). According to Dadas, 4 to 6% of all nasal polyps are antrochoanal type (1), sphenochoanal and ethmoidochoanal polyps are even more uncomom (3).
The cause of choanal polyps formation is not known. It is believed that they come from a cyst placed on paranasal sinus that grows gradually projecting itself through drainage ostium of its own paranasal sinus (5). Berg presented similarities between macro and microarquitecture of the intrasinusal component of choanal polyp and of the paranasal sinus cysts (5).
The target of this study is to present the case of a patient with progressive nasal obstruction complaints at right side. Its disgnostic investigation showed a large sphenochoanal polyp, which was completely removed through nasal endoscopy approach.
CLINICAL CASE PRESENTATIONThe patient was a black male student at his 13 years. He complained about progressive nasal obstruction at right side associated to a sensation of a ball in the throat for about a year and a half. He also complained about snoring and sleep apnea. He denied having otalgia (ear pain), dysphagia, anterior rhinorrhea, headache, allergy and/or epistaxis symptoms, but mentioned posterior rhinorrhea.
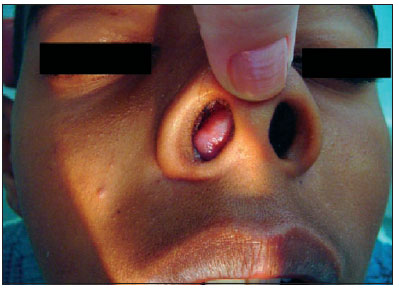
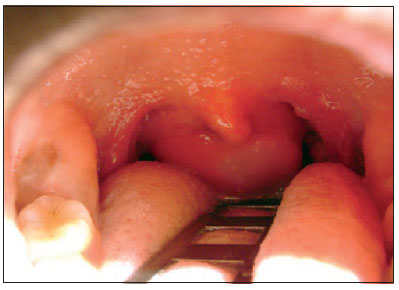
At anterior rhinoscopy and inspection (1), it was observed polyplike lesion, projecting itself through right nasal cavity. At oral-pharingoscopy (2) it was visualized large tumor coming from rhinopharynx filling almost all oral part of pharynx (oral-pharynx). It resembles the lesion described at anterior rhinophaynx.
It was impossible to have nasofibroscopy done from right nasal cavity due to the polyplike lesion in the place, impossible to visualize lesion at the left side due to septal deviation presence.
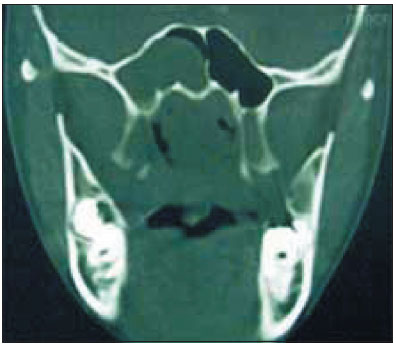
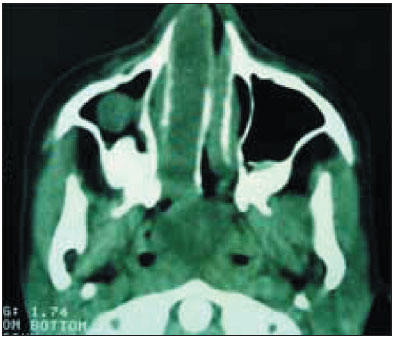
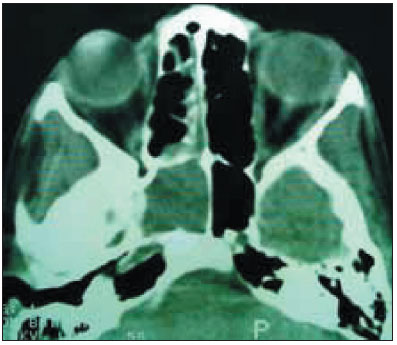
Computed tomography scan showed on coronary cuts there was uniform hiding on right sphenoid sinus and in almost all right nasal cavity, filling medial and lateral areas at right medium nasal concha and madial nasal at superior nasal concha and right inferior. Axial cuts showed uniform hiding on right sphenoid sinus, and hiding totally occupying rhinopharinx and oral-pharynx. It was impossible to observe natural drainage ostium enlargement of the right sphenoid sinus. As there were not any implications of other paranasal sinus, the likely diagnostic hypothesis was sphenochoanal polyp at right.
 Picture 1.
Picture 1. Anterior rhinoscopy and inspection.
 Picture 2.
Picture 2. Oroscopy.
It was suggested a surgical treatment through removal of ensonasal endoscopic. Sphenoethmoidal recess area was said to be identified at polyp implantation on anterior wall of right sphenoid sinus, besides enlargement of drainage ostium. It was done dissecation and removal of polyp implantation, through oral cavity because of its size. It was not placed any nasal packing after surgery and it did not occur anything negative during or after it. Patient was released from hospital 24 hours after surgery.
Histological exam of surgycal surgical specimen had inflammatory polyp as a result.
During follow-up of one, two, three and six months, it was not found any sign of recurrence, and patient did not have any nasal complaints.
DISCUSSIONSphenochoanal polyp is a rare disorder (1,3,6). It consist of solitary mass that arises from sphenoid sinus into the choana through its drainage ostium, going through sphenoethmoidal recess ocasionally reaching nasal-pharynx pushing inferior soft palate (1,7). They are different from nasosinusal polyposis as this one tends to be bilateral and composed by multiple polyps (8). This case patient presented large sphenochoanal polyp which occupied almost all oral-pharynx reaching the tongue basis (2).
Although some studies expressively mention the association between alergic diseases and choanal polyp formation, the reported patient did not have nasal alergic antecendent, so we may think this association is questionable (9).
Histologically, choanal polyps are similar. They are formed by a cystic center surrounded by oedema stroma which presents a kind of infiltration of inflammatory cells. Its surface is covered by respiratory epithelium (7) where areas of metapalsia can be found (6). MIN and col showed that eosinophilic infiltration (number of globet cells and submucosa glands) is more evident on choanal polyps rather than on nasal polyposis (10). Our patient presented inflammatory polyp as a result of histological exam.
Sphenochoanal polyp should be distinguished from meningoencephalocele (this presents imperfections on skull base that allows communication between cerebral and nasal cavities), nasopharyngeal angiofibromas (that present with recurrent epistaxis and enlargement of pterygomaxillary fossa in young patients), inverted papillomas (that in general present unilateral tumor with enlargement of ostiomeatal complex in older patients) among other nasal masses (3,7).
Its main differential diagnosis is with antrochoanal polyp, as they are clinical and histologically indistinctive (3). According to progressive growth, both types of choanal polyp are presented with unilateral nasal obstruction, facial pain and rhinorrhea, due to nasal cavity occupation and implication of ostiomeatal complex. These can be secondary otological symptoms to the lesions of ear tube, moreover snoring and sleep apnea obstruction due to rhinopharynx fulfillment. Both types of choanal polyps present the same incidence in both men and women under their 40s (3). The reported patient is a 13-year-old boy, and complained about progressive nasal obstruction at right for about eighteen months, so his history is compatible to choanal polyp. Although the large amount the tumor took on right nasal cavity as on rhino and oral-phariynx, the patient did not complain about dysphagia and/or symptoms related to ostiomeatal complex and/or ear tube implications. He complained about snoring, sleep apnea obstruction.
The distinction between antrochoanal and sphenochoanal polyps is very important both to avoid manipulation of paranasal sinus not involved on the disease and to reduce incidence of the appearing due to only simple traction of polyp without removing its implant (3,6). According to SOH & TAN (3) the best way to see the difference between the two polyps is through computed tomography scan and magnetic resonance imaging.
It is easy to determine, by imaging exam, if the origin place of polyp is on sphenoid or on maxillar sinus on isolated involvement cases of only one paranasal. Our patient presented implication only on the right sphenoid sinus, what allowed to establish the diagnosis of sphenochoanal polyp without any difficulty.
Therefore, the distinction of the two tumors is more difficult in case of there is opacification on both maxillar and sphenoid sinus at imaging exam (3). In order to see the difference on the origin place of polyp, we can use the following anatomic references: 1) Drainage ostium of maxillar and sphenoid sinus; 2) Sphenoethmoidal recess and medium meatus, and 3) Medium nasal concha (2,3).
 Picture 3.
Picture 3. C.T. (coronal): Uniform hiding on right nasal cavity.
 Picture 4.
Picture 4. C.T. (coronal): Uniform hiding on right sphenoid sinus and and on rhinopharynx.
 Picture 5.
Picture 5. C.T. (axial): Uniforme hiding on rhinopharynx and on right nasal cavity. Presence of cyst on right maxillar sinus.
 Picture 6.
Picture 6. C.T. (axial) Uniform hiding on right sphenoid sinus.
The drainage ostium enlargement of one of the paranasal sinus involved favors it as origin of polyp due to its expansive and erosive effect over its ostium (2,3). Analyzing sphenoethmoidal recess and medium meatus areas, we can suppose which is the origin place of tumor in case of one of these areas is occupied (2,3). Then, if hiding is placed at medium nasal concha in a lateral way, probably the polyp is antrochoanal. If hiding is placed in the middle, probably polyp is sphenochoanal (2,3).
We believe these analyzed signs all together are very important for diagnosis definiton, though, according to LOPATIN (11), nasofibroscopy, computed tomography scan and magnetic resonance imaging findings might not define the place of polyp implatation. On those cases, functional endoscopy surgery of paranasal sinus will be either diagnostic or therapeutic (11). Tomography cuts from the reported case did not permit to see the enlargment of drainage ostium of the sphenoid sinus. They pointed hiding on both lateral and medial area of right medium nasal concha (3). Yet, as mentioned before, there were no diagnosis difficulties, as right sphenoid was the only paranasal sinus involved (3,4,6). Spherical image on right maxillar sinus was not continuous on several tomography cuts, with nasal cavity hiding, what was a kind of cyst of maxillar sinus (5). This non-continous process was also present during surgery.
 Picture 7.
Picture 7. Surgical specimen
In relation to treatment of choanal and surgical polyps, TOSUN and col (7) report that almost 50% of sphenochoanal polyp in the literature occurred with children, so that the more aggressive surgical approaches (Caldwel-Luc, for instance) should be avoided, as the can cause facial asymmetry as long as they are growing patients. Endoscopy approach of choanal polyps has been more used (11) as it is effective and less aggressive than the external approaches.
Lopatin, besides confirming the effectiveness of endoscopy procedure, contests the basic concept of functional endoscopy surgery of paranasal sinus, saying that this concept is not applicable on choanal polyps. On functional endoscopy surgery of paranasal sinus the sick mucosa is not manipulated, as long as the improvement of drainage and aeration of paranasal sinus tend to restore normal mucosa of covering of this sinus). So, he suggests the removal of this sick mucosa since its presence might be recurrence. In the current case, polyp implant and adjancent sick mucosa to this implant were removed during surgical intervention with the purpose of reducing recurrence chances.
CONCLUSIONChoanal polyps are part of the diagnoses to be considered on progressive unilateral nasal obstruction approaches in children and young adults. Although antrochoanal is the most common type, the appearing on other paranasal sinus is possible and should be taken into consideration. In the sphenoid sinus case, it is important to do a differential diagnosis with other masses of this area.
The treatment of choanal polyps is surgical type. Endoscopy approach on this treatment has been used more and more, and it is diagnostic on those cases in which the imaging exams were not conclusive when differing antrochoanal and sphenochoanal polyps.
BIBLIOGRAPHY1. Dadas B, Yilmaz O, Vural C, Calis AB, Turgut S. Choanal polyp of sphenoidal origin. Eur. Arch. Otorhinolaryngol. 2000;257:379-381.
2. Weissman JL, Tabor EK, Curtin HD. Sphenochoanal Polyps: Evaluation with CT and MR Imaging. Radiology. 1991;178:145-148.
3. Soh KBK, Tan KK. Sphenochoanal Polyps in Singapore: Diagnosis and Current Management. Singapore. Méd. J. 2000;41(4):184-187.
4. Vangehuchten S, Bisschop P, Jortay A, Verbeurgt L. Diagnostic differentiel des masses du cavum chez l'adolescent. A propos d'um cas de polype antrochoanal. Acta Otorhinolaryngol. Belg. 1993;47:423-427.
5. Berg O, Carenfelt C, Silfversward C, Sobin A. Origin of the antrochoanal polyp. Arch. Otolaryngol. Head Neck Surg. 1988;114:1270-1271.
6. Crampette L, Mondain M, Rombaux Ph. Sphenochoanal polyp in children. Diagnosis and Treatment. Rhinology. 1995;33:43-45.
7. Tosun F, Yetiser S, Akcam T, Özkaptan Y. Sphenochoanal Polyp: endoscopic surgery Int. J. Pediatr. Otorhinolaryngol. 2001;58:87-90.
8. Voegels RL, Miyake MAM. Polipose Nasossinusal. In: Sociedade Brasileira de Otorrinolaringologia. Tratado de Otorrinolaringologia. 1ª ed. São Paulo: Roca, 2002, vol. 3, p. 88-99.
9. Cook PR, Davis WB, McDonald R, McKinsey JP. Antrochoanal polyps: a rewiew of 33 cases (see comments). Ear Nose Throat J. 1993;72:401-402. 404-410.
10. Min YG, Chung JW, Shin JS, Chi JG. Histologic structure of antrochoanal polyps. Acta Otolaryngol. 1995;115:543-547.
11. Lopatin A, Bykova V, Piskunov G. Choanal polyps: One entity, one surgical approach? Rhinology 1997;35:79-83.