 |
563 |
|
| Year: 2008 Vol. 12 Num. 4 - Out/Dez - (4º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Pattern of Otological Diseases in School Going Children of Kathmandu Valley |
|
| Author(s): |
| Prakash Adhikari1, Dr. Binit Kharel2, Jasmine Ma2, Dipak Raj Baral2, Tilchan Pandey2, Rajendra Rijal2, Hariom Sharma2
|
|
|
| Key words: |
| otological diseases, school children, Kathmandu |
|
|
 |
| Abstract: |
Introduction: Ear disease in children is a major public health concern in developing countries. In spite of availability of potent antibiotics, severe life threatening complications of ear diseases can occur. Objective: This study was done to find out the prevalence of different types of otological disease in school going children of Kathmandu valley. Method: This is prospective study among 1245 school children aged between 5-12 years in the time period of June 2007 - May 2008. Students were randomly selected from 4 different schools of Kathmandu valley. All these children were interviewed, examined otoscopically and findings were noted in the performa. Informed consent was taken from guardians to participate in this study. Statistical analysis was done using frequency and percentage. Results: Out of 1245 children, 64.0% were male and 36.0% female children. The most common otological diseases were wax (60.6%), followed by chronic suppurative otitis media (5.7%) and otitis media with effusion (3.7%). In CSOM, there was 85.9% tubotympanic type. Overall otological diseases were present in 75.7% children. Conclusion: There is a high prevalence of otological diseases in school going children of Kathmandu valley. Health education, improvement of socioeconomic status and health facilities will be helpful in reducing the prevalence of otological diseases.
|
|
|
INTRODUCTION
Preventable ear diseases have been found to be important health problems among children (1). Nearly one third of Otorhinolaryngology outdoor attendance in the hospital comprised of paediatric age group. The problem is compounded by the fact that the children are economically dependent on their parents who are largely poor. This tends to delay early presentation to the hospital. In spite of availability of potent antibiotics, severe life threatening complications of ear diseases. Diseases of the ear can be diagnosed usually by taking a very good history. Asking the patients leading questions about the disorders of the sensory systems and the related structure is helpful in diagnosis (2). Such leading questions include the presence or absence of the following symptoms: otalgia, otorrhoea, hearing impairment, high grade fever, tinnitus, vertigo, deep seated headache, pre or post auricular swelling and facial paralysis. Adequate examination of the entire child with special attention to the head and neck, can lead to the identification of a condition that may predispose to or be associated with ear disease (3).
There are only few documented studies of the prevalence of chronic suppurative otitis medial in Nepal. But no such studies are published in medical literature regarding otological diseases in school going children of Nepal. However, comparison of findings of one study with that of others poses difficulty as the age group studies and the methodology used in these studies are viewed. So, this study was done to find out the prevalence of different types of otological disease in school going children.
METHOD
This is prospective study among 1245 school children aged between 5-12 years in the time period of June 2007 - May 2008. Students were randomly selected from 4 different schools of Kathmandu valley. All these children were interviewed, examined otoscopically and findings were noted in the performa. Children with blue drum, thickened, dull and opalescent or thin and reflective drum with increased vascularity with or without fluid levels and decreased mobility were labeled as otitis media with effusion. Informed consent was taken from guardians to participate in this study. Statistical analysis was done using frequency and percentage.
RESULTS
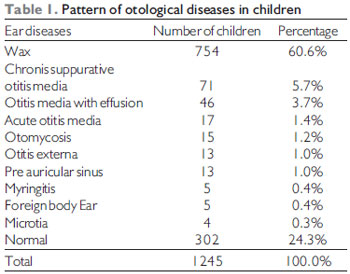
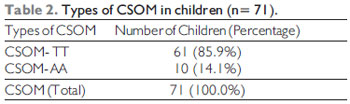
Out of 1245 children, 64.0% were male and 36.0% female children. The most common otological diseases were wax (60.6%), followed by chronic suppurative otitis media (5.7%) and otitis media with effusion (3.7%) (Table 1). In CSOM, there was 85.9% tubotympanic type (Table 2). Overall otological diseases were present in 75.7% children.
DISCUSSION
Ear disease in children is a major public health concern in developing countries. The World Health Organization suggests that, in developing countries, children should be screened at school entry using a simple audiometer and that the external ear be inspected for the presence of discharge, to study the extent of the problem in the community (4).
This study indicates that ear diseases in school going children is a considerable burden in Kathmandu valley. It is not surprising that wax (60.6%) in our study obstructing the tympanic membrane is relatively common, because in the majority of cases it is asymptomatic and therefore not an indication for seeking medical care. Hatcher et al (5), Mann et al (6), Elango et al (7) and Minza et al (8) study reported prevalence rates of impacted wax ranging from 8.6% to 28.2%. Okafor et al study however found wax impaction to be the third most common ear disease in the southeastern part of Nigeria (9). However, the high prevalence of impacted wax in the present study could be due to the fact that the study was restricted to children of age 5-12 years, unlike the above mentioned studies which have included children of higher age groups.
Impacted wax is mostly a silent condition and may not have been attended to by the caregivers of the children of school entry age and possibly had influence on hearing. Sharma et al (10) and Jacob et al (11) study reported wax as the most common cause of hearing impairment, which accounted for 50 and 29.8% of cases respectively.
Chronic suppurative otitis media (CSOM) is a major health problem throughout the world in developing countries including Nepal (12). It is the most common cause of persistent mild to moderate hearing impairment in children and young adults (13). High rates of CSOM have been attributed to overcrowding, inadequate rates of nasopharyngeal colonization with potentially pathogenic bacteria and inadequate or unavailable health care (13). Poverty is a major risk factor in developing countries and certain neglected populations (14). Previous studies done by Adhikari et al in Kathmandu valley revealed that 5.7% of children from government school and 4.8% of children from private school had CSOM (12). However, this study showed that 5.7% of children had CSOM. The prevalence of CSOM in our study was found to be similar to the prevalence quoted by Rupa et al (15) (6%) and Olege et al (6.0%) (16) but lower than the study done by Maharjan et al (17) (13.2%), Biswas et al (13) (12.4%) and Morris et al (18) (15.0%). Akinpelu et al study showed that a very high prevalence (33.9%) of CSOM in Nigerian children (2). Almost all of our school children had tubotympanic type (85.9%) of disease which is lower than the findings of Adhikari et al (12).
Otitis media with effusion (OME) is the commonest cause of hearing impairment and one of the most frequent reasons for elective admission to hospital for surgery during childhood. OME also known as middle ear effusions, frequently persist for a short time following episodes of AOM although 90% of such effusions have resolved within 3 months (19). The exact prevalence of this disease in Nepal is not known. Study done in Nigeria revealed that 5.3% of children had OME which is slightly higher than our study (2).
Acute otitis media or acute suppurative otitis media (AOM/ASOM) is an episode of inflammation of the middle ear associated with pain, fever, hearing loss and sometimes discharge. Sixty five to 95% of children will have suffered one or more attacks before the age of 7 years (20). ASOM was the third most common ear diseases in a study done by Akinpelu et al, which accounts for 7.0% cases (2). However, our study revealed that 1.4% of school going children of Kathmandu valley had AOM. It was also the fourth most common ear disease in our children.
Otomycosis, otitis externa, myringitis, foreign bodies and congenital malformations of ear are least common diseases in descending order in our study. However, Akinpelu et al study revealed foreign body in the ear as the 5th common ear disease (2). Among the congenital malformations of ear preauricular sinus was the most common.
On the overall, there was a high prevalence (75.7%) of otological diseases in school going children of Kathmandu valley. Although the observed prevalence of ear disease may not reflect exactly the true prevalence in the community, it gives an indication of what may be expected. Prevalence of ear disease within the community may be higher than the observed in this study, since those children with hearing impairment and/or disease may be less likely to attend school compared to their healthy colleagues.
CONCLUSION
Preventable ear diseases are important health problems among school going children of Kathmandu valley. Wax followed by chronic suppurative otitis media and otitis media with effusion were the most common otological diseases in children. There is a high prevalence of otological diseases in these children. Health education, improvement of socioeconomic status and health facilities will be helpful in reducing the prevalence of otological diseases. Provision of at least one primary ear care assistant to every school, if not otherwise in one village, can be one suitable option to reduce the disease.
REFERENCES
1. Rao RS, Subramanyam MA, Nair MS, Rajashekar B. Hearing impairment and ear diseases among children of school entry age in rural south India. Int J Paediatr Otorhinolaryngol. 2002, 64:105-10.
2. Akinpelu OV, Amusa YB. Otological diseases in Nigerian children. The Internet J Otorhinolaryngol. 2007, 7:1.
3. Bluestone CD, Klein JO. Methods of examination: clinical examination. In: pediatric otolaryngology.2nd edn. Philadelphia; 1990, 111-4.
4. Gell FM, White E, McNewell K, Mackenzie I, Smith A, Thompson S et al. Practical screening priorities for hearing impairment among children in developing countries. Bull. World Health Org. 1992, 70:645-55.
5. Hatcher J, Smith A, Mackenzie I, Thompson S, Bal I, Macharia I et al. A prevalence study of ear problems in school children in Kiambu district, Kenya, May 1992. Int J Pediatr Otorhinolaryngol. 1995, 33:197-205.
6. Mann S.B.S., Bhardwaj A, Gudi SP, Mehra YN, Incidence of speech, hearing and ENT problems in school-going children, Hearing Aid J. 1985, 2:39-42.
7. Elango S, Purohit GN, Hashim M and Hilmi R. Hearing loss and ear disorders in Malaysian school children. Int J Pediatr Otorhinolaryngol. 1991. 22:75-80.
8. Minja BM and Machemba A. Prevalence of otitis media, hearing impairment and cerumen impaction among schoolchildren in rural and urban Dar es Salaam, Tanzania. Int J Pediatr Otorhinolaryngol. 1996, 37:29-34.
9. Okafor BC. Otolaryngology in Southeastern Nigeria: pattern of diseases of the ear, Nigeria Medical Journal. 1983, 13:11-9.
10. Sharma H, Bhusan V, Dayal D and Mishra SC. Preliminary study of hearing handicap in school-going children. Indian J Otolaryngol Head Neck Surg. 1992, 30:119-24.
11. Jacob A, Rupa V, Job A and Joseph A. Hearing impairment and otitis media in a rural primary school in South India. Int J Pediatr Otorhinolaryngol. 1997, 39:133-8.
12. Adhikari P. Chronic suppurative otitis media in school children of Kathmandu valley. Int Arch Otorhinolaryngol. 2007, 11:175-8.
13. Biswas AC, Joarder A H, Siddiquee BH. Prevalence of CSOM among rural school going children. Mymensingh Med J. 2005, 14:152-5.
14. Prevention of Hearing impairment from chronic otitis media, WHO/CIBA foundation workshop report. London. 1996, 19-21.
15. Rupa V, Jacob A, Joseph A .Chronic suppurative otitis media: Prevalence and practices among rural south Indian children. Int J Pediatr Otorhinol. 1999, 48:217-21.
16. Ologe FE, Nwawol CC. Prevalence of chronic suppurative otitis media (CSOM) among children in a rural community in Nigeria. Niger Postgrad Med J. 2002, 9:63-6.
17. Maharjan M, Bhandari S, Singh I, Mishra SC. Prevalence of otitis media in school going children in eastern Nepal. Kath Uni Med J. 2006, 16:479-82.
18. Morris PS, Leach AJ, Silberberg P et al. Otitis media in young Aboriginal children from remote communities in Nouthern and central Australia; a cross sectional survey. BMC Pediatr. 2005, 5:27.
19. D Teele, J Klein Rosner B. Epidemiology of otitis media in children. Annals Otorhinolaryngol (Suppl). 1980, 89:5-6.
20. Claessen JQPJ, Appelman CLM, Toluw-otten FWM, de Meeker RA, Hordijik GJ. A review of clinical trials regarding treatment of acutt otitis media. Cl Otolaryngol. 1992, 17:251-7.
1. Doctor. President, Healthy Human Society, Jorpati, Kathmandu, Nepal.
2. Doctor. Member, Healthy Human Society, Jorpati, Kathmandu, Nepal.
Institution: Healthy Human Society, Jorpati, Kathmandu, Nepal. Kathmandu, Nepal.
Address for correspondence:
Dr. Prakash Adhikari
President - Healthy Human Society
Jorpati, Kathmandu - Nepal - PO Box: 4972
E-mail: healthy_hs@hotmail.com / prakash_ooz@hotmail.com
Article received in September 19, 2008.
Article approved in November 27, 2008.
|
|
 |
|
|
