 |
578 |
|
| Year: 2008 Vol. 12 Num. 4 - Out/Dez - (19º)
|
|
 |
|
|
| Myxoma of Cervical Soft Tissue: Case Report and Literature Review |
|
| Author(s): |
| Giulianno Molina de Melo1, Tiago Vieira Tavares2, Thomaz Antonio Fleury Curado2, Giancarlo Bonotto Cherobin2, Gabrielle do N. Holanda Gonçalves2, Cristiane M. de F. Ribeiro3
|
|
|
| Key words: |
| myxoma, neoplasms of connective tissue |
|
|
 |
| Abstract: |
Introduction: Myxomas are benign mesenchymal tumors that rarely occur in the head and neck area. Most of these injuries are odontogenic and involve facial bones. Myxomas of the soft tissue are very rare and widely distributed in the body, and most frequently reported in the heart muscles. Objective: To describe a case of extramuscular soft tissue myxoma in the left submaxillary area. Case Report: A male patient was referred to our service with extramuscular soft tissue myxoma in the left submaxillary area initially behaved as a branchial cyst. The treatment consisted of surgical excision with adequate margins and subsequent histology confirmation of the myxoma. Conclusions: The adequate resection of extramuscular myxoma is the main choice to avoid local failure, and the follow-up must be rigorous.
|
|
|
INTRODUCTION
The term myxoma was initially described by Virchow (1), in 1871, when he observed tumors that histologically were similar to the umbilical cord mucinous tissue. In 1948, Stout (2) reported 49 patients with myxoma and established a diagnosis criterion: a true mesenchymal neoplasm, formed exclusively from undifferentiated star-shaped cells, in a loose mucoid stroma, that don't result in metastasis. Since then, the myxomas have been seen as uncommon and as locally connective tissue benignant infiltrative tumors that appear both in the bone and in the soft tissues.
In the head and neck region, the myxomas occur normally in the jaw, maxillary and soft tissues of the face (3). Extramuscular soft tissue myxomas in the cervical region are uncommon and only some cases are described in the English literature (4).
The objective of this report is to present a case of cervical extramuscular myxoma and the literature review.
CASE REPORT
A 65-year-old, male sex, white, alcoholic and smoker patient sought our service in April 2004 with a history of left cervical region tumoration of four years with progressive growth. In the physical exam he presented with cystic and single node in the left submandibular region, with approximately 5.0 cm of diameter. It was mobile, painless to palpation and without phlogistic signals. No cervical lymphonodomegalia was observed. The remaining physical exam (oroscopy, indirect laryngoscopy and thyroid gland palpation) was within normality.
The neck computerized tomography confirmed the cystic ovular formation, with 4.2 cm of diameter, located in the left submandibular lodge with projection to the tonsillar lodge (Picture 1). The (FNAB) fine-needle aspiration biopsy guided by ultrasonography revealed the absence of neoplasic cells. The diagnostic hypothesis of branchiogenic cyst was then considered and we therefore discarded the squamous cell carcinoma metastasis or thyroid gland carcinoma metastasis. The treatment consisted of the mass surgical excision, with margins deemed to be wide for branchiogenic cyst resection without rupture during the excision.
 Picture 1. Cervical Soft Tissue Myxoma - Computerized Tomography of the Neck with left submandibular cystic lesion.
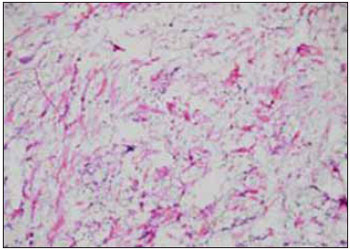
The lesion was sent for macroscopic analysis, which confirmed the ovoid part, with 5.0 g of weight, 6.0 x 4.0 x 2.0 cm of measure and surface partially covered by fleshy tissue. To the cuts, we remarked a node with 5.5 cm of diameter with cystic central area filled with colorless gelatinous material. The remainder of the node was soft and gray. Sequential cuts were made with the usual techniques for inclusion of paraffin and coloration. The histological study described a mesenchymal tumor, with fusiform cells without atypias, surrounded by abundant mucoid material, that filled the myxoma diagnosis criteria (5) (Pictures 2 and 3).
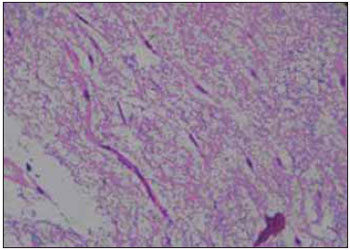 Picture 2. Myxoma histology - Mesenchimal Neoplasm with abundant colloid in the fusiform cells proliferation. 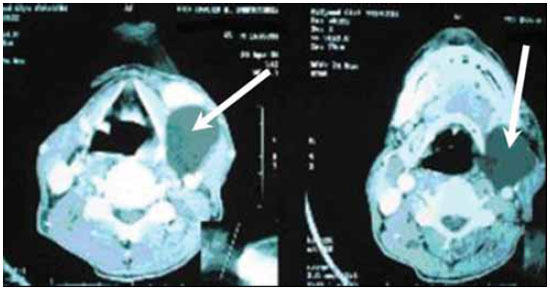 Picture 3. Myxoma Histology - Mesenchimal Neoplasm with fusiform cells proliferation without atypias.
The patient evolved without intercurrences in the postoperative period, was discharged from hospital the day after and receives service follow-up for physical and radiologic exams with computerized tomography, initially in the period of every six months during two years and then annually with exams, without evident recurrence in the four-year follow-up so far.
DISCUSSION
The myxoma etiology remains unknown. Most authors agree the myxomas are derived from a primitive embryonal mesenchyme or fibroblasts able to produce mucopolysaccharides in abundance (6). Its most common appearing place in the organism is the heart, followed by the thigh and shoulder myxomas (7).
In the head and neck region, the myxomas originate normally in the bones (61%), specially the jaw and maxilla, and are very common in the adult population (3). Soft tissue myxomas are found in several parts of the organism, and may be divided into: intramuscular myxoma, juxta-articular myxoma, superficial angiomyxoma, aggressive angiomyxoma and neurothekoma (nervous sheath myxoma) (8). The intramuscular myxoma occurs generally in middle-aged women and are commonly located in the thigh, shoulders, gluteal region and upper limb muscles.
The juxta-articular myxoma is histologically similar to the intramuscular myxoma, but it affects the periarticular tendons, ligaments, joints, muscles and subcutaneous tissue in adults (8). The superficial angiomyxoma, also known as cutaneous myxoma, occurs in all ages, with a slight prevalence in the third and fourth decades of life and appears commonly in the trunk, lower limbs and head and neck region.
The aggressive angiomyxoma normally affects the pelvis and the perineum and is seven times more frequent in the female sex with a recurrence rate reaching about 50% of the cases (8). The neurothekoma occurs more frequently in the upper ends and the head and neck regions of young women (9).
In the bone tissue or in soft tissue, the myxomas are usually identified in the intra-operative as a gelatinous mass of oval or spherical shape, mucoid appearance and variable consistency (3). Its fibrous capsule is normally incomplete and reaches the adjacent tissues. The histopathology reveals star-shaped cells with eosinophilic cytoplasm and small core. These are separate by an abundant mucoid extracellular stroma that may be vacuumed and present with cystic change (5).
The extramuscular myxoma differential in the cervical region must be made with the most common cystic tumors of the neck, such as the branchiogenic cyst, laryngocele, spinocellular carcinoma cystic metastasis and thyroid papilliferous carcinoma cystic metastasis.
The choice treatment must be the surgical excision with free margins, which thus prevents recurrences. It's presumable that part of the tumor eradication difficulty is based on the poor definition of its margins (3). The conservative treatment is indicated only in lesions close to vital structures, mainly in young patients. Other types of treatment were proposed (enucleation, removal, radiotherapy), but with high levels of recurrence and further wide surgical resection.
This report's patient is without evidence of recurrences so far, from the control image and physical exam.
CONCLUSION
The extramuscular soft tissue myxoma in the cervical region is an uncommon benignant neoplasm, of infiltrative nature, whose diagnosis is made after histopathologic analysis. The choice treatment must be the surgical removal with wide margins, which thus prevents recurrences and the rigorous service follow-up.
BIBLIOGRAPHICAL REFERENCES
1. Virchow R. Die cellularpathologie in ihrer Beegrundung auf physiologische and pathologische Gewebelehre. Berlin, Germany, Verlag von August Hirschwald. 1871, 563.
2. Stout AP. Myxoma, the tumor of primitive mesenchyme. Ann Surg. 1948, 127:706-719.
3. Andrews T, Kountakisse, Maillard AA. Myxomas of the head and neck. Am J Otolariyngol. 2000, 21:184-9.
4. Galera-Ruiz H, Martin-Gomez R, Esteban-Ortega F, Congregado-Loscertales M, Garcia Escudero A. Extramuscular soft-tissue myxoma of the lateral neck. Rev Laryngol Otol Rhinol. 2001, 122:259-61.
5. Fletcher CDM, Unni KK, Mertens F (Eds). World Health Organization Classification of Tumors. Pathology and Genetics of tumors of Soft tissue and Bone. IARC Press: Lyon, 2002.
6. Enziger FM. Intramuscular myxoma. Am J Chin Pathol. 1965, 43:104-13.
7. Ghosh BC, Huvos AG, Gerald FP, et al. Myxoma of the jawbones. Cancer. 1973, 3:237-40.
8. Allen PW. Myxoma is not a single entity: a review of the concept of myxoma. Ann Diagn Pathol. 2000, 4:99-123.
9. Papadopoulos EJ, Cohen PR, Hebert AA. Neurothekoma: report of a case in an infant and review of the literature. J Am Acad Dermatol. 2004, 50:129-34.
1. Master's Degree-FMUSP; TCBC-SP. Assistant of Head and Neck Surgery of the Head and Neck Surgical Service of the Hospital Beneficência Portuguesa de São Paulo.
2. Resident Otorhinolaryngologist of the Otorhinolaryngology Service "Ivan Fairbanks Barbosa" of the Hospital Beneficência Portuguesa de São Paulo.
3. Pathologist of the Pathology Integrated Center - Hospital Beneficência Portuguesa de São Paulo.
Institution: Hospital da Beneficência Portuguesa de São Paulo. São Paulo / SP - Brazil
Mail address:
Giulianno Molina de Melo
Rua Dr. Luis Migliano 761, Apto 84-B - Morumbi
São Paulo / SP - Brazil - Zip code: 05711-001
Fax: (+55 11) 3683-2401 and 3283-4591
E-mail: giulianno_molina@hotmail.com
Article received on November 16, 2007.
Approved on July 3, 2008.
|
|
 |
|
|
