 |
614 |
|
| Year: 2009 Vol. 13 Num. 2 - Abr/Jun - (12º)
|
|
 |
|
|
| How Can the Cochlear Implant Interfere with the Vestibular Function? |
|
| Author(s): |
Patricia Arena Abramides1, Ricardo Ferreira Bento2, Roseli Saraiva Moreira Bitar3,
Rubens Vuono de Brito Neto4, Robinson Koji Tsuji5
|
|
|
| Key words: |
| cochlear implant, dizziness, Ménière's disease. |
|
|
 |
| Abstract: |
Introduction: The cochlear implant is a therapeutic option for patients with deep neurosensorial deafness. Some implanted patients evolved with dizziness in the postoperative, which started the interest for the vestibular function. Since then, many studies have reported the association between the cochlear implant and the vestibular dysfunctions.
|
|
|
INTRODUCTION
Hearing is the function that helps us understand the world around us. The presence of the hearing capacity was fundamental for the survival of our species: getting around from predators, the crying of the suckling, the calling of the group. However, what differs the general living beings from humans is the tireless search for a means that allows us not only living more, but living with quality. And hearing has a basic importance in the so dreamed quality of life. It was aiming at rescuing this function that several researchers dedicated to the development of some interface that could recover the sound perception to those who lost it or never had it.
The cochlear implant (IC) is a prosthesis aiming at replacing the affected organ of Corti, by directly stimulating the nervous fibers and the ganglionar cells of the auditory nerve. This option enables the auditory sensation and the speech and sound recognition.
Differently from the hearing aid, that requires the existence of hair cells to transfer the signal to the auditory nevus, the cochlear implant takes over the function of such cells and activates the auditory nerve directly. Then, by using the CI, the individual with severe and deep hearing loss is able to perceive auditory sensations.
The interest for the vestibular function in implanted patients started with the observation that some of them evolved with dizziness in the postoperative. Since then, several authors dedicated to the research and documentation of the vestibular system function in these patients.
The objective of this study is to review the current knowledge concerning the vestibular function in patients with CI.
METHOD
The first article that addresses the subject was written by Black in 1977 (1). From then, a survey in the literature has found 40 articles regarding the vestibular function in patients with CI. The bibliographic research was made between 1970 and May 2008, in the following databases: PUBMED, MEDLINE, LILACS, OVID.
The keywords used for the search were: cochlear implant, vertigo, dizziness, Ménière's disease The articles were selected according to inclusion criteria: articles published in English; articles that related CI with the vestibular system and the body balance study; articles that addressed dizziness relating to the CI surgery. We excluded articles written in other languages rather than English and those from magazines not published in Brazil.
Our research focus comprised: the presence and the type of involvement of the vestibular function and the anatomic description of the vestibular-cochlear interaction.
RESULTS
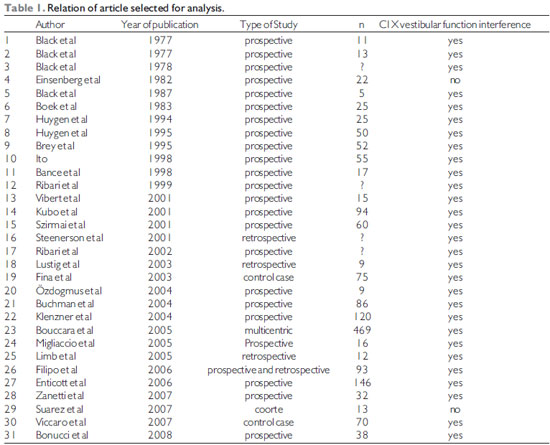
Out of 40 articles found, 31 met the inclusion criteria. Nine articles were excluded for meeting the exclusion criteria. 5 for having been published in papers that are not published in Brazil and 4 for having been published in other language (1 article in Japanese, 1 in German, 1 in Russian and 1 in Polish).
In Table 1 you find 30 reported articles that med the inclusion criteria and were selected for analysis.
DISCUSSION
Since Black (1977) (1, 2) described a reduction or absence of the answers in the caloric proofs of patients submitted to CI, many other studies reported the potential risk of the cochlear implant to interfere with the vestibular function (3, 4, 5, 6).
The articles studied presented a variable general quality. In 4 articles we didn't even set up the number or group of the patients studied (see articles with ?). Most authors carried out a prospective study from the observation of patients submitted to CI who presented some complaint regarding body balance during its evolution. Even though, in many studies the variable "time" was not well defined. The number of patients studied ranged from 5 to 469, which makes it difficult and, to a certain extent, not much reliable to set up a pattern of comparison between the various results found. Other difficulty was to group the studies around a common point, since they presented different objectives. The authors used different evaluation criteria of the vestibular function, since questionnaire, such as the dizziness handicap inventory (DHI), activities-specific balance confidences (ABC); electronistagmography (ENG), video-oculography (VOG), use of force platforms, computer dynamic posturography (CDP), descending pendular rotatory test (DPRT), Dix-Hallpike maneuver and even criteria for Ménière's disease. The evaluation criteria were the same before and after surgical interventions, except for Bonucci, who used the caloric proofs from water in the preoperative and air in the postoperative; which makes the adequate and reliable results analysis difficult.
Out of 31 authors, 16 chose ENG isolated or combined with other exams for evaluation of the vestibular function. Buchman et al (2004) were the only authors to use ENG, Computer Dynamic Posturography DPRT, and DHI jointly, and presented a complete and reliable study regarding preoperative and postoperative vestibular function (14).
From our research focus we may infer that as for the vestibular function, the opinions of the authors are controversial. Some believe that CI interferes with the vestibular function and has a risk of loss ((Brey, Vibert, Enticott, Huygen and Steenerson) (3, 6, 25, 28, 31) and others believe CI has no effect on vestibular function (Einsenberg, Migliaccio AND Suarez) (19, 23, 24). In the other hand, there are authors who believe the CI may improve body balance (Buchman, Szirmai, Bance and Ribari) (14, 15, 16, 38).
The risk of vestibular function loss was variable for Huygen et al (6, 39). While such risk was estimated in 31% in the first study (6), in a second sample the same author reports the risk between 50-60% of post cochlear implant vestibular function loss (39). His last study is according to the results of Van Den Broek et al (40), who found 60% of risk of post-CI vestibular function loss. However, Bouccara et al (4) found 16% of the adults and 3% of the children who presented dizziness at the CI postoperative. For Vibert (28) et al the canalicular function was temporarily damaged in 20% of the cases while the otolithic function was preserved in all the 6 patients tested.
According to Suarez (24) et AL, the alterations on the balance didn't remain and, in spite of this vestibular function loss, the children could keep an adequate balance control, and CI doesn't affect the sensorial organization strategy.
Another group of authors believes the CI doesn't cause balance risk, such as Einsenberg et al and Migliaccio et al. Bance et al (19,23,38), believed it's possible that the multichannel CI activates the vestibule-ocular system in some cases, but in a clinically non-significant manner. Opinion shared by Buchman et al (14), who believe the patients submitted to CI may have a significant improvement of the posture evaluated by the Computer Dynamic Posturography. If we analyze the period of follow-up carried out by each author, we verify that Buchman (14) performed serial evaluation in 30 days, 4 months, 1 year and two years after CI, while Migliaccio followed the patients for 4 to 6 weeks after the CI. Einsenberg (19) and Bance (38) did not set up the follow-up period. That is, the "time" factor was determining to define the CI influence to the vestibular function. The work by Buchman (14), who studied the major period of follow-up, described the improvement of the vestibular function. Therefore, the studies with a short or undefined follow-up period may not be taken into account upon determination of the real influence of the entire work of stimulation and fitting of the CI for body balance.
Out of the 60 patients studied by Szirmai et al (16), 16 had a vestibular response improvement at the postoperative, whose explanation is not clear for the author. For Ribari et al (1999) both the auditory and the vestibular improvement of the ear contralateral to CI may be ascribed to 2 factors: Efferent innervation and brain plasticity. In 2002, the same author (15) reported a hearing and response improvement to the caloric test of the non-implanted ear in 30% of the cases. The author concludes that such observations may be explained by the neuronal plasticity and the auditory stimulus may affect the labyrinth.
As for the complications occurred in the CI postoperative, we also find controversy in the literature. For Filipo et al (20), the CI may induce to vestibular damage right after its placing or activation, which could be a possible complication of the intraoperative trauma or, at a lower degree, the electric stimulation. According to Enticott (3), one third of the patients may present some disorder of the vestibular system after CI and apparently the oldest patients are more prone to permanent vestibular damages.
Fina et al (21) reported that in 39% of the implanted patients who presented with dizziness, it occurred lately and could be a result from changes in the inner ear such as endolymphatic hydrops. For Kubo (22), the inner ear lesions secondary to CI develop gradually and are clinically comparable to the Ménière's Syndrome, which indicates the presence of labyrinthic hydrops. According to Lustig et al (27), patients with Méniére's Disease, previously submitted to the vertigo control surgery (neurectomy, endolymphatic sac decompression) don't present contraindication for IC, which could benefit them from the audiologic point of view.
For Brey et al (25), most symptoms in the postoperative are transient, but when persistent, the treatment indicated is vestibular rehabilitation. For Klenzner et al (29), the risk of vestibular disorder after the CI surgery is reduced by the atraumatic insertion of electrodes.
Amongst the vestibular disorders described, the benign paroxist postural vertigo is a problem remarked in the literature as a post-CI complication. The relationship between this vertigo (VPPB) and CI was studied by Limb et al (26), Viccaro et al (32) and Zanetti et al (36). According to the first two authors the vertigo (VPPB) does not usually occurs after CI, but has a major incidence than in the general population. The treatment consists of repositioning maneuvers as it's usually done, and according to Zanetti (36), the VPPB does not interfere with the patients' speech perception.
According to studies carried out by Black et al, between 1977 and 1978 (1, 2, 18), the CI stimulates the vestibular nucleus through electric current and, therefore, the stimulus generated is not only limited to the auditory system. We observed instability when the patients were evaluated with the CI on, which suggests the action on the vestibular system. According to the author (1987) (34), the auditory, vestibulocolic and vestibulospinal reflexes confirmed their dependence upon the stimulus duration, frequency and amplitude. According to Ito (5), there was dizziness in 18% of the cases when the CI was activated; which indicates the electric current generated by the CI reaches the vestibular nerve.
Recently, Özdogmus et al (13), showed connections between the lower and cochlear vestibular nerves fibers and between the upper and facial vestibular nerves by means of electronic microscopy. The descriptions of connections between the vestibular and auditory systems may justify some clinical findings observed in implanted patients.
CONCLUSION
There are clinical evidences that CI is able to interfere with the vestibular function. The type of functional alteration is marked by anatomic factors, for individual predisposition to the stimulus pattern produced by the CI and also by the plastic capacity of the neural system of each individual.
BIBLIOGRAPHICAL REFERENCES
1. Black FO. Present vestibular status of subjects implanted with auditory prothesis. Ann Otol Rhinol Laryngol. 1977, 86(Suppl 38):49-56.
2. Black FO. Effects of the auditory prothesis on postural stability. Ann Otol Rhinol Laryngol. 1977, 86(Suppl 38):141-164.
3. Enticott JC, Tari S, Koh SM, Dowell RC, O'Leary SJ. Cochlear implant and vestibular function. Otol Neurotol. 2006, 27(6):824-30.
4. Bouccara D, Esteve Fraysse MJ, Loundon N, Fraysse B, Garabedian N, Sterkers O. Vestibular dysfunction after cochlear implantation: a national multicenter clinical study. Rev Laryngol Otol Rhinol (Bord). 2005, 126(4):275-8.
5. Ito J. Influence of the multichannel cochlear implant on vestibular function. Otolaryngol Head Neck Surg. 1998, 118(6):900-2.
6. Huygen PL, Hinderink JB, Van Den Broek P, Van Den Borne S, Brokx JP, Mens LH, Admiraal RJ. The risk of vestibular function loss after intracochlear implantation. Acta Otolaryngol Suppl. 1995. 520 Pt 2:270-272.
7. Burian M, Gstoettner W, Zundritsch R. Saccular afferent fibers to the cochlear nucleus in the guinea pig. Arch. Otolaryngol. 1989, 246:238-241.
8. Rasmussen AT. Studies of the VIII'th cranial nerve of man. Laryngoscope. 1940, 50:67-83.
9. Arnesen AR. Fiber population of the vcestibulocochlear anastomosis in humans. Acta Otolaryngol. 1984, 98:501-518.
10. Kim HS, Kim DI, Chung IH, Lee WS, Kim KY. Topographical relationship of the facial and vestibulocochlear nerves in the subarachnoid space and internal auditory canal. AJNR Am J Neuroradiol. 1998, 19:1155-1161.
11. Silverstein H. Cochlear and vestibular gross and histologic anatomy (as seen from pstauricular approach). Otolaryngol. Head Neck Surg. 1984, 92:207-211.
12. Nageris B, Braverman I, Kalmanowitz M, Segal K, Frenkiel S. Connections of the facial and vestibular nerves: na anatomic study. J Otolaryngol. 2000, 29:159-161.
13.Özdogmus Ö, Sezen O, Kubilay U, Saka E, Durman U, San T, Cavdar S. Connections between the facial, vestibular and cochlear nerve bundles within the internal auditory canal. J Anat. 2004, 205:65-75.
14. Buchman CA, Joy J, Hodges A, Telischi F, Balkany T. Vestibular Effects of Cochlear Implantation. The Laryngoscope. 2004, 114(10 part 2):1-22.
15. Ribari O, Szirmai A, Kustel M, Repassy G. How does cochlear implantation affect the contralateral vestibular system? Int Tinnitus J. 2002, 8(2):108-10.
16. Szirmai A, Ribari O, Repassy G. Air caloric computer system application in monitoring vestibular function changes after cochlear implantation. Otolaryngol head Neck Surg. 2001, 125(6):631-4.
17. Ribari O, Küstel M, Szimari A, Repassy G. Cochlear implantation influences contralateral hearing and vestibular responsiveness. Acta Otolaryngol. 1999, 119(2):225-8.
18. Black FO, Wall C 3rd, Oleary DP, Bilger RC, Wolf RV. Galvanic disruption of vestibulospinal postural control by cochlear implant devices. J Otolaryngol. 1978, 7(6):519-27.
19. Eisenberg LS, Nelson JR, House WF. Effects of the single-electrode cochlear implant on the vestibular system of the profoundly deaf adult. Ann Otol Rhinol Laryngol Suppl. 1982, 91(2 Pt 3):47-54.
20. Filipo R, Patrizi M, La Gamma R, D'Elia C, La Rosa G, Barbara M. Vestibular Impairment and cochlar implantation. Acta otolaryngol. 2006, 126(12):1266-74.
21. Fina M, Sskinner M, Goebel JA, Piccirillo JF, Neely JG, Black O. Vestibular dysfunction after cochlear implantation. Otol Neurotol. 2003, 24(2):234-42.
22. Kubo T, Yamamoto K, Iwaki T, Doi K, Tamura M. Different forms of dizzness occuring after cochlear implant. Euro Arch Otorhinolaryngol. 2001, 258(1):9-12.
23. Migliaccio AA, Della Santina CC, Carey JP, Niparko JK, Minor LB. The vestibulo- ocular reflex response to head impulses rarely decreases after cochlear implantation. Otol Neurotol. 2005, 26(4):655-60.
24. Suarez H, Angeli S, Suarez A, Rosales B, Carreara X, Alonso R. Balance sensory organization in children with profound hearing loss and cochlear implants. Int J Pediatr Otorhinolaryngol. 2007, 4251:1-9.
25. Brey RH, Facer GW, Trine MB,Lynn SG, Peterson AM, Suman VJ. Vestibular effects asociated with implantation of a multiple channel cochlear prothesis. Am J Otol. 1995, 16(4):424-30.
26. Limb CJ, Francis HF, Lustig LR, Niparko JK, Jammal H. Otolaryngol Head Neck Surg. 2005, 132(5):741-745.
27. Lustig LR, Yeagle J, Niparko JK, Minor LB. Cochlear implantation in patients with bilateral Ménière's syndrome. Otol Neurotol. 2003, 24(3):397-403.
28. Vibert D, Häusler R, Kompis M, Vischer M. Vestibulat function in patients with cochlear implantation. Acta Otolaryngol Suppl. 2001, 545:29-34.
29. Klenzner T, Neumann M, Aschendorff A, Laszig R. Laryngorhinotologie. 2004, 83(10):659-64.
30. Himi T, Shintani T, Yamaguchi T, Harabuchi Y, Kataura A. Vestibular function in cochlear implants - prognostics factors and postoperative damage. Nippon Jibiinkoka Gakkai Kaiho. 1995, 98(7):1111-1118.
31. Steenerson RL, Cronin GW, Gary LB. Vertigo after cochlear implantation. Otol Neurotol. 2001, 22 (6):842-843.
32. Viccaro M, Mancini P, La Gamma R, De Seta E, Covelli E, Filipo R. Positional vertigo and cochlear implantation. Otol Neurotol. 2007, 31.
33. Mangnusson M, Petersen H, Harris S, Johansson R. Postural control and vestibular function in patients selected for cochlear implantation. Acta Otolaryngol Suppl. 1995, 520 Pt 2:277-8.
34. Black FO, Lilly DJ, Fowler LP, Simmons FB. Vestíbulo-ocular and vestibuloespinal function before and after cochlear implant surgery. Ann Otol laryngol Suppl. 1987, 96(1 Pt 2 suppl 128):106-8.
35. Himi T, Shintani T, Yamaguchi T, Harabuchi Y, Kataura A, Yoshioka I. Relation between vestibular function and speech recocgnition in postlingually deafened adults with cochlear implantation. Áudiol Neurootol. 1997, 2(4):223-30.
36. Zanetti D, Campovecchi CB, Balzanelli C, Pasini S. Paroxysmal positional vertigo after cochlear implantation. Acta otolaryngol. 2007, 127(5):452-8.
37. Rossi G, Solero P, Rolando M, Spadola Bisetti M. Vestibular function and cochlear implant. ORL J Otorhinolaryngol Relat Spec. 1998, 60(2):85-87.
38. Bance ML, O'DRiscoll M, Giles E, Ramsden RT. Vestibular stimulation by multichannel cochlear implants. Laryngoscope. 1998, 108(2):291-294.
39. Huygen PL, Van Der Broek P, Spies TH, Mens LH Admiraal RJ. Does intracochlear implantation jeopardize vestibular function? Ann Otol Rhinol Laryngol. 1994, 103(8Pt 1):609-614.
40. Van Der Broek P, Huygen PL, Spies T, Mens LH, Admiraal RJ. Vestibular function in cochlear implant patients. Acta Otolaryngol. 1993, 113(3):263-265.
41. Bonucci AS, Costa Filho OA, Mariotto LDF, Amantini RCB, Alvarenga KF. A função vestibular em indivíduos usuários de implante coclear. Rev Bras Otorrinolaringol. 2008, 74(2):273-278.
1. Specialist Doctor in Otorhinolaryngology.
2. Professor of the Otolaryngology Department, FMUSP.
3. PhD in Medicine from the University of Sao Paulo. Assistant Physician, Department of Otolaryngology HCFMUSP
4. Associate Professor, FMUSP. Assistant, Division of Clinical Otorhinolaryngology HCFMUSP
5. PhD in Otorhinolaryngology by FMUSP. Attending Physician, Division of Clinical Otorhinolaryngology HCFMUSP Coordinator of the Cochlear Implant Team HCFMUSP
Institution: Departamento de Otorrinolaringologia da FMUSP ICHC. São Paulo / SP - Brazil
Mail address:
Patricia Arena Abramides
Departamento de Otorrinolaringologia da FMUSP ICHC
Avenida Enéas de Carvalho Aguiar 255, 6º andar - Sala 6021
São Paulo / SP - Brazil - CEP: 05403-000
Telephone: (+55 11) 8271-0138
E-mail: parena@terra.com.br
Article received on June 30 2008.
Accepted on March 28 2009.
|
|
 |
|
|
