 |
640 |
|
| Year: 2009 Vol. 13 Num. 3 - Jul/Set - (18º)
|
|
 |
|
|
| Nasoendoscopic Treatment of the Sphenoid Sinus Mucoceles |
|
| Author(s): |
| Paulo Tinoco1, José Carlos Oliveira Pereira2, Rodolfo Caldas Lourenço Filho2, Fabrício Boechat do Carmo Silva3.
|
|
|
| Key words: |
| sphenoid sinus, mucoceles, amaurosis. |
|
|
 |
| Abstract: |
Introduction: Mucoceles is a slow growth benign lesion, composed of mucous or purulent material, may be multiple and cause osseous erosion. The sphenoid sinus mucoceles are uncommon and correspond to 1% of the cases; they are more frequent in the frontal and ethmoidal sinuses respectively. Objective: To report one case of sphenoid sinus mucoceles that occurred with neurological symptoms and was submitted to surgical treatment through nasal endoscopy. Case Report: 80-year-old female patient with a record of ocular pain, diplopia and progressive decrease of the visual accuracy, which evolved with bilateral amaurosis two months after. In the cranium CT and MR we confirmed an expansive mass of sphenoid sinus, suggesting mucoceles. The patient was submitted to nasoendoscopic surgery with opening and widening of the ostium in the sphenoid sinus. Final Comments: The pathologies that affect the sphenoid sinus represent a great importance due to the noble structures that surrounds it. The nasal endoscopic surgery is an excellent approach for the treatment of mucoceles.
|
|
|
INTRODUCTION
The paranasal sinuses mucoceles are benign expansive cystic lesions that occur more commonly in the frontal and ethmoidal sinuses and they are rare in the sphenoid sinus (1). The mucocele is characterized clinically by a silent initial period, of undetermined duration, followed by a period in which its expansion causes deformity and complications. The high resolution Computed Tomography (CT) and the Nuclear Magnetic Resonance (NMR) are the choice diagnosis exams (2). The treatment is surgical and may be approached with conventional methods or by nasal endoscopy (3). In this article we describe the case of a patient with sphenoid sinus mucocele (SSM) and neurological symptoms.
CASE REPORT
A.C.S., 80 years old, female sex, retired, born in São José de Ubá - RJ, sought the Neurology Service of HSJA with complaint of "blindness". She reported ocular pain, dyplopia and progressive decrease of the visual accuracy, that evolved with bilateral amaurosis two months later. The cranial CT revealed a mass that emerged form the sphenoid sinus and compressed the ocular innervation. She was forwarded to the Otorhinolaryngology service, that raised a strong suspicion of sphenoid mucocele. The NMR confirmed the said expansive mass (Pictures 1 and 2) suggesting mucocele. The patient was submitted to nasoendoscopic surgery with opening and enlargement of the sphenoid sinus ostium (Pictures 3 and 4). She was followed up weekly through nasal endoscopy and presented a complete improvement of the algic picture, but with a low improvement of the visual accuracy.
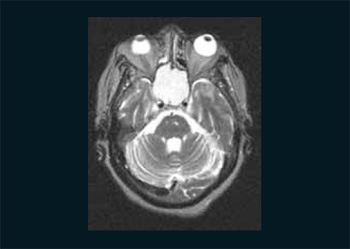 Picture 1. NMR in axial cut showing expansive mass of the sphenoid sinus.
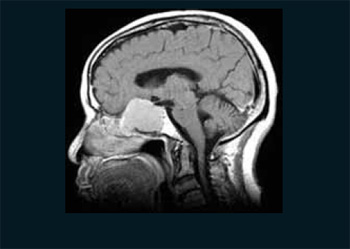 Picture 2. NMR in sagital cut showing expansive cystic mass occupying the sphenoid sinus and compressing the adjacent structures.
 Picture 3. Right nostril: Opening of the sphenoid sinus. Middle infundibulum on the right, nasal septum on the left and opening of the sinus with the help of a nipper in the center.
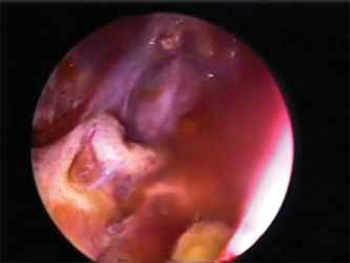 Picture 4. Endoscopic view of the sphenoid sinus roof. Transparency view of the internal carotid artery.
DISCUSSION
The mucocele is defined as an expansive cystic formation resulting from the accumulation and retention of mucous secretion in the paranasal sinus, that occur when the sinus draining is obstructed (1). Its incidence is higher in the third and fourth decades of life, without predilection for sex (4). In about 60% of the cases, the mucoceles are secondary to surgical procedures in the facial sinuses, in 35% of the cases they are primary and 2% are traumatic. The sphenoid sinus, the less commonly involved, represents 1% to 8% of the paranasal mucoceles (5). Despite it is benign, its expansive nature may slowly cause erosion of the paranasal sinuses osseous limits by compression and consequent osseous reabsorption, which leads to commitment of adjacent structures (6). This is what occurred in the case described, in which the structures adjacent to the sphenoid sinus were compressed, and led to the symptomatology described.
The clinical manifestations of the SSM are variable and the most common are headache, ophthalmoplegia, decrease of the visual accuracy, anosmia and signs of nasal obstruction. More severe conditions, such as cerebral abscess, meningitis and amaurosis may be part of the picture (1). In our case, the patient reported ocular symptoms of insidious evolution that resulted in bilateral amaurosis for compression of the optic chiasma.
The mucoceles differential diagnosis is made with Rathke's cyst, cysticercosis, dermoid cyst, hypophisary adenoma, craniopharyngeoma, optic glioma, as well as the neoplasm lesions of the cranial base, face sinuses and nasopharynx (2).
The cranial CT is considered to be the choice exam, because it allows the viewing of the level of sinusal expansion, osseous destruction and the involvement of adjacent structures. In addition, it is possible to make the differential diagnosis with neoplasms, since the mucocele does not undergo any enhancement with the administration of contrast (7). It generally demonstrates an encapsulated and well delimited cystic mass , that may invade adjacent structures. The NMR supplies a better information about the commitment of the optic nerve and the carotid artery caused by the disease. The large mucoceles may eventually be similar to sinusal neoplasms in the CT, while NMR may easily differ a tumoral extension from the accumulation of secretion resulting from an obstruction of the sinusal ostium. Its use is not common and is recommended when the CT shows the presence of osseous erosion, when the mucocele expands outwards the sinus and also when there is partial or total vision loss (8). The treatment of mucoceles is surgical and the access way may be conventional methods (transcranial and transeptal) or nasal endoscopy. It aims at diagnostic confirmation, draining and excision or masurpialization of the cyst's wall (3).
In this case, we opted for the endonasal access by videoendoscopy for it is a functional not much invasive approach and of low morbidity and the lesion broad masurpialization and draining are carried out, by preserving the surface epithelium. A rigorous postoperative follow up is necessary. Frequent cleaning of the mucocele cavity and of nasal cavities help in the prevention of inflammation and the recurrent disease. Routine endoscopic evaluations are made in the patient's evolution. Computed tomography or magnetic resonance may be necessary, specially in case of suspicion of recurrence (9).
FINAL COMMENTS
The pathologies affecting the sphenoid sinus are very important due to the noble structures that surround it and many times manifest with neurological symptoms.The endoscopic surgery is an excellent means of approach for the treatment of mucoceles. We believe in the case described there was no important improvement of the visual accuracy due to the long period in which the vascular and nervous structures were compressed.
BIBLIOGRAPHIC REFERENCES
1. Abe T, Ludecke D. Mucocele like formation leading to neurological symptons im prolactina secreting pituitary adenomas under dopamine agonist therapy. Surg Neurol. 1999, 52:274-79.
2. Gondim J, Pinheiro I, Junior OIT. Tratamento neurocirúrgico da mucocele esfenoidal pela via nasoseptal transesfenoidal endoscópica: relato de dois casos. Arq. Neuropsiquiatr. 2002, 60(2-A):299-302.
3. Caylakli F, Yavuz H, Cajici A, Ozlvoglu LN. Endoscopic sinus surgery for maxillary sinus mucoceles. Head & Face Medicine. 2006, 29(2):1-5.
4. Ifbal J, Kanaan I, Ahmed M, et al. Neusurgical aspests sphenoid sinus mucocele. Br J Neurosurg. 1998, 12:527-530.
5. Rombaux P, Bertrand B, Eloy P, et al. Endoscopic endonasal surgery for paranasal sinus mucoceles. Acta Otorrinol Belg. 2000, 54:115-122.
6. Kennedy D.W, Josephson J.S, Zinreich S.J, Mattox D.E, Goldsmith M.M. Endoscopic sinus surgery for mucoceles: a viable alternative. Laryngoscope. 1989, 99:885-95.
7. Som PM, Shugar JMA. Antral Mucoceles: A new lok. J Comput Assist Tomogr. 1980, 4:484-488.
8. Gilain L, Aidan D, Coste A, Peynegre R. Functional endoscopic sinus surgery for isolated sphenoid sinus disease. Head & Neck. 1994, 16:433-7.
9. Nicolai P, Luca O, De Zinis R, Tomenzoli D, Maroldi R, Antonelli. Sphenoid mucocele with intracranial invasion secondary to nasopharyngeal acinic cell carcinoma. Head & Neck. 1991, 13:540-4.
1. Specialist in Otorhinolaryngology. Coordinator of the Medical Residence Service in Otorhinolaryngology of Hospital São José do Avaí.
2. Resident in Otorhinolaryngology of HSJA.
3. Trainee of the Otorhinolaryngology Service of HSJA.
Institution: Hospital São José do Avaí Itaperuna / RJ - Brazil. Mail Address: Paulo Tinoco - Rua Coronel Luiz Ferraz, 397- Centro - Itaperuna / RJ - Brazil - Zip code: 28300-000 - Telephone: (+55 21) 3822-2836 - E-mail: paulo_tinoco@ig.com.br
Article received on July 9 2008. Article accepted in May 10, 2009.
|
|
 |
|
|
