|
650 |
|
| Year: 2009 Vol. 13 Num. 4 - Out/Dez - (7º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Analysis of the Vocal Health of the Preachers of the Seventh-Day Adventist Churches |
|
| Author(s): |
Francisco Xavier Palheta Neto1, Itaiana Pereira Cordeiro da Silva2, Aniele Vilarino Madeira3, Christiane do Rosário Teixeira Menezes4,
Lorena Gonçalves Rodrigues5, Larissa Magalhães Navarro6.
|
|
|
| Key words: |
| voice disorders, hoarseness, risk factors, quality of life, worker's health, voice. |
|
|
 |
| Abstract: |
Introduction: The dysphonia cases are common in professions that use the voice continuously. Out of these, we find the preachers who are submitted to several vocal alterations for the abusive use of the voice. Objective: To analyze the occurrence of laryngeal symptoms in the preachers of the Seventh-Day Adventist Churches in the city of Belém and to alert for the problem. Method: We carried out a prospective, individualized and transversal study through the completing of a research-owned questionnaire. We evaluated 56 preachers, according to acceptance. Results: The 56 preachers were male with mean age of 35.8 years. As for the occupation, only 8 (14%) exerted other activities that also demanded the occupational use of the voice. This study showed that the activity time average of the preachers was of 10.2 years. As for the vocal cares, only 29 (51.7%) practiced vocal cares, of whom 13 (7.2%) carried out vocal warm-up before their activities. The triad of clinical symptoms of major frequency was: Clearing of the throat, observed in 44 preachers (78.5%), hoarseness, in 32 (57.1%) and pain/irritation, in 29 (51.8%). As for the habits and lifestyle only one (1.8%) preacher reported he had the habit of smoking, one (1.8%) informed he used marijuana and two (3.7%) mentioned they drank alcoholics. Conclusion: We observed a high prevalence of vocal complaints in the preachers studied. Clearing of the throat was the most frequent (78.5%), followed by hoarseness (57.1%) and laryngeal pain/irritation (51.8%). These professionals' instruction and training as for the cares regarding the vocal health could reduce the high prevalence o such complaints.
|
|
|
INTRODUCTION
The voice plays an essential role in communication and human relationships, and improves the transmission of articulated messages, by adding to the word the emotional content, intonation and expressivity and identifying the individuals as well as their physiognomy and their digital impressions. Nowadays, there are professions that require the individuals to use their voices continuously, such as, singers, teachers, radio speaker, actor and pastor. We call these individuals who use their voices in the professional performance voice professionals (1).
In Brazil, the official statistics show that 25% of the economically active population consider the voice to be a primary work instrument and depend on it to exert some type of occupation or turn it into their living element. There are estimates that about 25 thousand professionals will be deprived of their work for problems in the larynx and vocal cords (2).
Dysphonia may occur as a result of an interaction between hereditary, behavioral, organic and occupational factors. Several studies have related the occupational activity to dysphonia. We believe the main factor is related to the excessive use of the voice, which causes a trauma on the vocal cords. However, it is worth pointing out several environmental factors that may be relating to work and indirectly contribute for the problem, such a: exposure to chemical irritants, bad condition of temperature and humidity, background noises and bad environmental conditions. In addition to this, the limited time of recovery and stress is also considered to be risk factors for the occupational laryngopathy. Factors relating to the lifestyle may also be harmful to the voice (3).
Therefore, this study was accomplished with the general objective to analyze the occurrence of vocal disorders in pastors of the Seventh-Day Adventist Church in the state of Pará, aiming to identify, among other characteristics, the clinical complaints and the life habits of this group, and alert for the problem.
METHOD
All pastors involved in this research were interviewed according to the principles of the declaration of Helsinki and Nuremberg Code, by complying with the Researches involving human beings (Res. CNS 196/96) of the National Council of Health, after approval by the Ethics Committee in Research. The interviewee took part in the research after signing the Free and Clarified Authorization Term.
For this study we collected clinical, personal and professional information, as well as their habits, through a proper questionnaire prepared by the researchers. We interviewed 56 pastors, all from the Seventh-Day Adventist Churches, located in cities of the State of Pará, in May 2008. This a prospective, individualized, observational and transversal study defined as an epidemiological inquiry.
The selection of professionals who took part in this study was made according to individual acceptance. The interviewees were benefited with the clarification of doubts about this theme at the moment of data collection, when a lecture was held on vocal care. We excluded the interviewee who were under phonotherapeutic treatment. No complimentary exams were carried out because most of the pastors did not live in the capital city and were in the city only temporarily.
The data collected included: For how long they exerted the function of pastor, working time in a day of major vocal activity, average weekly working time, professional performance in other activity with the excessive use of the voice, additional working time due to such activity; information about smoking, alcoholics, use of drugs, sports practice, instruction about vocal health in the church or elsewhere; clinical symptomatology (throat pain or irritation, hoarseness, sensation of foreign body, presence of clearing of the throat, neck pain) use of medications. We emphasize that for ethical reasons, the identity of all participants in the research was preserved.
The data collected was stored in a database, in the Bio Estat 4.0 program. The results were analyzed according to frequency descriptive statistics as for the program mentioned, according to the objectives proposed for the work.
RESULTS
The study included 56 pastors of the Seventh-Day Adventist Church, all of the male sex. We obtained the following distribution of interviewees as for the age range: 31 (55.4%) were in the age range from 31 to 40 years, 15 (26.8%) between 20 to 30 years, and groups from 41 to 50 years and older than 50 years added 5 (8.9%) interviewees each, as described in Graphic 1.
As for the time of work as pastor, we confirmed that: 22 (39.4%) exerted the activity for less than 5 years, 15 (26.7%) between 6 and 10 years, 6 (10.7%) between 11 and 15 years and 13 (23.2%) over 15 years, as described in Graphic 2.
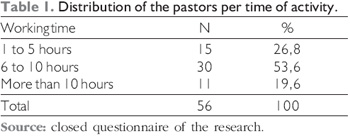
The daily work working time indicated that 15 pastors (26.8%) exerted their activities during less than five daily hours, 30 (53.6%) between 6 and 10 hours, and 11 (19.6%) worked on the activity for more than 10 hours a day (Table 1).
Concerning the exercise of other professional activity, we detected that 48 (86%) interviewees dedicated exclusively to the religious activity and 8 (14%) exerted another activity.
The most reported clinical symptomatology was: Clearing of the throat, by 44 (78.5%) of the interviewees, hoarseness in 32 (57.1%) and sensation of pain and irritation in the throat in 29 (51.8%), as described in Graphic 3.
Among the pastors that reported hoarseness, in only 4 (13%) the symptom was constant, and in 52 (87%) hoarseness was episodic, always related to vocal use/abuse moments.
As for the habit of water drinking, we verified that 37 (66%) pastors drank less than two liters of water per day, while 19 (34%) ingested a higher quantity.
Upon correlation of the main symptoms observed to the daily water drinking, we observed a major prevalence of hoarseness in those who drank less than two liters compared to the group who drank more water during the day. A total of 5 pastors (8.9%) did not present symptomatology, no matter the volume ingested.
Only 1 (1.8%) pastor reported having the habit of smoking, one (1.8%) informed he consumed marijuana and two (3.7%) reported the use of alcoholic drinks. One group of 33 (59%) mentioned they practiced sports.
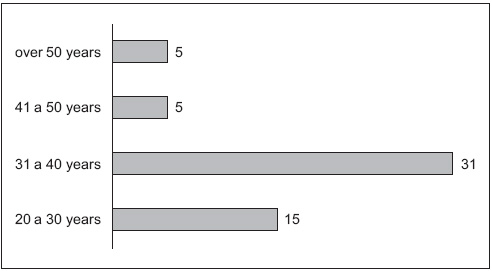 Graphic 1. Distribution of pastors by age range. - Source: closed questionnaire of the research.
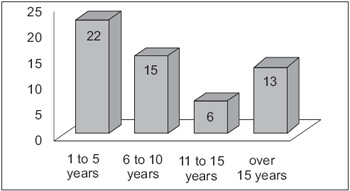 Graphic 2. Distribution of the pastors per time of activity. - Source: closed questionnaire of the research.
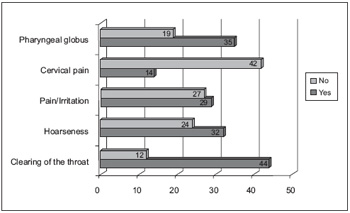 Graphic 3. Description of the referred clinical symptomatology. - Source: closed questionnaire of the research.
DISCUSSION
The importance of voice for the human communication is unquestionable, and it has an essential role in the work market, specially for professionals who use it as their main instrument of work activity (3, 4). Among these professionals, we may mention: teachers, actors, singers, receptionists, telemarketing operators, lawyers, pastors, health professionals, etc. For them, dysphonia may represent the impossibility to exercise their profession, which causes damages to work, diminishing of income and even the need for change of profession (3, 5).
The professional attribution of a protestant pastor is not restricted to the preaching of cults, but he also dedicates himself for religious teaching, singing of religious anthems, work as a spiritual counselor and church administrator, that is to say, he represents the ecclesiastical government. For DUARTE (1997) the pastor is truly a voice athlete (6). Therefore we verify that the voice is active in all of their duties. Thus, the work of the otorhinolaryngologist is of large importance for the phonation apparatus, aiming to prevent and treat the voice pathologies and dysphonia, that are consequences of lack of knowledge, by the pastors, and to decrease the vocal damages.
Dysphonia may be a multifactorial cause and a consequence of association with factors such as: hereditary, behavioral, lifestyle and occupational aspects. Several studies have been relating the occupational activity to dysphonia and we believe the main factor is bound to the excessive use of the voice, which causes trauma in the vocal cords and inflammatory processes, with laryngitis as the most frequent one (2, 7). Environmental factors may be related to the appearing of the problem: improper conditions of temperature and humidity, noises, chemical irritants exposure (such as chromium, mercury, formaldehyde, sulphuric acid), and an acoustics unsuitable to the environment (1, 8).
In a study involving pastors, LIMA (2001) (9) verified that 50% of his research presented some vocal complaint after religious cult. In the research protocol, the most reported clinical symptomatology was: clearing of the throat, present in 44 (78.5%) of the interviewees, hoarseness in 32 (57.1%), and sensation of pain or irritation in the throat, 29 (51.8%). Among the pastors that reported hoarseness, in only 4 (13%) the symptom was constant, and in their majority, 52 (87%) hoarseness was episodic, always related to vocal use/abuse moments. For COLTON & CASPER (1996) (10), the abusive voice behavior results from the excessive and prolonged intensity that may lead to the vocal quality: blowing, hoarse, rough voice, breakings of the voice, aggravated pitch, vocal fatigue, voice dynamics extension reduction, inadequate breathing standard and muscle-skeleton tension syndromes.
Dysphonia is common in voice professionals and has been not much valued during too long. Today it is taken as an important disorder, with consequences that directly influence the professional and social life, lately deemed to be an occupational problem, since it diminishes the productivity and regularity in the work of these professionals (11, 12, 13). In addition to this, the limited time of recovery and stress is also considered to be risk factors for the occupational laryngopathy. With the association between the presence of symptoms and the daily activity working time, we verified that most of those who reported a positive symptom had their daily activities performed for a period longer than 6 hours a day. Opposite to our results, in a study with another group of voice professionals (teachers), SAPIR (1993) 13 did not verify any association between the frequency of dysphonia and their working time as voice professionals.
The factors relating to the lifestyle may also be harmful to the voice (3). Amongst these, we may cite smoking, excessive alcoholic drinks, laryngopharyngeal reflux (8). In our study we note that, only 1 (1.8%) pastor reported having the habit of smoking, one (1.8%) informed he consumed marijuana and two (3.7%) reported the use of alcoholic drinks. We ascribed this low incidence to the religious concepts, to which the participants of this study are bound. One group of 33 (59%) mentioned they practiced sports.
It is known that to carry on a suitable clinical follow-up in this type of patient, prevention programs are important for possible vocal cords lesions, as well as guidance about the early recognition of the symptoms related to a good vocal hygiene. This includes avoiding irritating agents, such as active or passive smoking, suitable diet, laryngopharyngeal reflux control, of dust and proper water drinking (1, 16). As for the latter factor, we verified that 37 (66%) pastors drank less than two liters of water per day, while 19 (34%) ingested a higher quantity. Upon correlation of the main symptoms observed to the daily water drinking, we observed a major prevalence of hoarseness in those who drank less than two liters, 32 (57.2%). We consider water drinking to be essential for the maintenance of vocal quality, which matches the findings of our studies (17, 18).
For BOMPET and SARVAT (1998), the need for an interrelation between the phonoaudiologist and the laryngologist is highly important, with a mutual trust of the technical and scientific knowledge and professional conduct, since they are both faced with a voice professional (19). The otorhinolaryngologist treats with medication, surgical and preventive procedures, in case the pastor does not present with any organico-functional symptom of the phonation apparatus. The phonoaudiologist will treat with a procedure based on the otorhinolaryngologist's diagnosis and the voice evaluation, in the pastor's vocal behavior and with the detailed anamnesis of the vocal parameters, and will guide about vocal hygiene and phonotherapy for enhancing of the voice use.
CONCLUSION
We observed a high prevalence of vocal complaints in the pastors studied. Clearing of the throat was the most frequent (78.5%), followed by hoarseness (57.1%) and laryngeal pain/irritation (51.8%). These professionals' instruction and training as for the cares regarding the vocal health could reduce the high prevalence o such complaints.
BIBLIOGRAPHICAL REFERENCES
1. Soares EB, Brito CMCP. Perfil vocal do guia de turismo. Rev CEFAC. 2006, 8(4):501-8.
2. Palheta-Neto FX, Pezzin-Palheta AC. Voz: a necessidade do cuidado permanente. Jornal Diário do Pará. Belém - Pará, Jul. 2004.
3. Carding P. Managing dysphonia caused by misuse and oversuse. BMJ. 2000, 32:1544-5.
4. Satalof RT. Evaluation of professional voice singers. Otolaryngol Clin N Am. 2000, 33:923-55.
5. Ingram DB, Lehman JL. Management of high-risk performers in clinical practice. Curr Opin Otolaryngol Head Neck Surg. 2000, 8:143-52.
6. Duarte N. Você pode falar melhor. Rio de Janeiro, JUERP, 1997. 145p
7. Fortes FSG, Imamura R, Tsuji DH, and Sennes LU. Perfil dos profissionais da voz com queixas vocais atendidos em um centro terciário de saúde. Rev Bras Otorrinolaringol. 2007, 73(1).
8. Feijó A. Disfonia Funcional, Brasil, 1999. Disponível em http://www.fonoaudiologia.org.br/JORNAL/04/j4-5.htm. Acessado em: 03/08/2009
9. Lima BM. A voz do pastor evangélico. Rev CEFAC. 2001.
10. Colton RH, & Casper JK. Compreendendo os problemas de voz: uma perspectiva fisiológica ao diagnóstico e ao tratamento. Porto Alegre: Artes Médicas. 1996.
11. Ferreira JB, Ferreira DS. Estudo descritivo de 451 atendimentos na campanha da semana nacional da voz. Rev Bras Otorrinolaringol. 2001, 67(1):90-93.
12. Roy N, et al. Voice disorders in teachers and the general population. J Speech Lang Hear Res, 2004b, 47(3):542-551.
13. Ortiz E. Saúde vocal de professores da rede municipal de ensino de cidade do interior do interior de São Paulo. Rev Bras Med Trab. 2004, 2(4):263-266.
14. Sapir A, Keidar A, Mathers-Schmidt B. Vocal Attrition in Teachers: Survey Findings. Europ J Disord Commun. 1993, 28:177-85.
15. Carmo JC. Distúrbios de voz relacionados ao trabalho. BEPA. 2006, 3(26):1-21.
16. Pinho SMR. Manual de higiene vocal para profissionais da voz. Carapicuíba: Editora Pró-Fono, 2003.
17. Solomon NP, Glaze LE, Arnold RR, Mersbergen M. Effects of a vocally fatiguing task and systemic hydration on mens voices. J Voice. 2003, 17:31-46.
18. Yiu EM, Chan RMM. Effect of hidration and vocal rest on the vocal fatigue in amateur karaoke singers. J Voice. 2003, 17:216-27.
19. Bompet R & Sarvat MA. Importância do trabalho integrado na área de voz. In. Pinho SMR. Fundamentos em Fonoaudio-logia. Rio de Janeiro. Guanabara Koogan, 1998. P.44-8.
1. Master's Degree in Otorhinolaryngology at UFRJ. Doctoral Degree in Neurosciences at UFPA. Assistant Professor of Otorhinolaryngology at UEPA and UFPA. Preceptor of the Medical Residence in Otorhinolaryngology in the Medical School Betina Ferro de Souza of UFPA.
2. Resident of the Second Year at the Medical School Bettina Ferro de Souza. Federal University of Pará - UFPA.
3. Fifth Year Medical Student Federal University of Pará - UFPA.
4. Phonoaudiologist at the Otorhinolaryngology Center of Pará and the Otorhinolaryngology Service of the Medical School Betina Ferro de Souza. Master's Degree in Neuroscience and Cellular Biology. Specialist in Language, Public Health and Voice.
5. Resident of the First Year of Otorhinolaryngology at the Medical School Bettina Ferro de Souza. Federal University of Pará
6. Resident in Otorhinolaryngology at the Medical School Bettina Ferro de Souza. Federal University of Pará - UFPA.
Institution: Otorhinolaryngology Center of Pará. Belém / PA - Brazil. Mail Address: Francisco Xavier Palheta Neto - Centro de Otorrinolaringologia do Pará - Avenida Conselheiro Furtado, 2391, Salas 1508 e 1608 - Edifício Belém Metropolitan - Bairro: Cremação - Belém / PA - Brazil - Zip code: 66040-100 - Telephone: (+55 91) 3249-9977 / (+55 91) 3249-7161 / (+55 91) 9116-0508 - E-mail: franciscopalheta@hotmail.com. Article received on September 26 2009. Approved on November 29 2009.
|
|
 |
|
|