 |
712 |
|
| Year: 2010 Vol. 14 Num. 3 - Jul/Set - (15º)
|
|
 |
|
|
| Non-syndromic Keratocystic Odontogenic Tumor Involving the Maxillary Sinus: Case Report |
|
| Author(s): |
| Gustavo Davi Rabelo1, João Cesar Guimarães Henriques1, José Humberto Macedo2, Claudia Jordão Silva3, Sergio Vitorino Cardoso4, Adriano Mota Loyola5, Antônio Francisco Durighetto Junior6.
|
|
|
| Key words: |
| odontogenic tumors, maxillary sinus, radiology, surgery. |
|
|
 |
| Abstract: |
Introduction: The odontogenic keratocyst tumor is rarely found in maxilla. Case Report: This article describes a report of a case of a 60-year-old Caucasian female with an asymptomatic growth in the region of the posterior maxilla tumor diagnosed as odontogenic keratocyst. We discuss the diagnosis and workup for this type of injury.
|
|
|
INTRODUCTION
Odontogenic keratocyst is the traditional term used to describe a benign but locally aggressive odontogenic cystic lesion with distinctive clinical and histopathologic features (1). World Health Organization proposed the term "keratocystic odontogenic tumor" (KOT) to reflect the neoplastic nature of this lesion (2).
LITERATURE REVIEW
Keratocystic odontogenic tumors almost certainly arise from derivatives of the dental lamina, an embryonic structure that normally differentiates into tooth buds and enamel-producing cells during odontogenesis (3). This lesion shows features of both a cyst and a benign neoplasm (4). Albeit eventually associated to nevoid basal cell carcinoma syndrome, most of KOT occur as sporadic lesions.
Up to one-fourth from all of KOT affect the maxilla, but maxillary sinus involvement is very rare (5,6). In a retrospective study of 183 cases, the mandible was the site of occurrence of 70.5% of tumors and 16.4% occurred in the maxilla, however, 13.1% occurred in both (7).
Radiographically, it appears as a well-defined lucency and is often multilocular. KOTs represent 5-15% of all odontogenic cysts and the recurrence rate for solitary KOT is 10-30% (8).
The aim of this paper was describe an intriguing case of a patient with a non-syndromic KOT involving maxillary sinus and discuss the pathogenesis of the disease, highlighting recent molecular data obtained from it.
CASE REPORT
A 60 year-old Caucasian female presented with an asymptomatic growth in the right posterior maxilla. It was present for sixteen years and the patient reported eventual gingival bleeding and mild pain. Past medical and familiar history was noncontributory. Oral examination revealed a firm swelling with normal overlying mucosa. Panoramic radiograph (Figure 1) evidenced a well defined 4cm round unilocular lesion effacing the right maxillary sinus. Also, sclerotic areas of mixed density were found in premolar and molar regions of the mandible in the right side, with a very suggestive aspect of benign fibro-osseous lesions (Figure 2). Axial and coronal computerized tomography images delineated a hypodense spherical lesion in the right maxilla with extension to the sinus, suggesting a cystic alteration (Figure 3). Aspiration with a 29-gauge needle obtained yellowish and viscous liquid, suggesting keratin content. Incisional biopsy was performed and histopathology confirmed the diagnosis of KOT (Figure 4). The lesion was then enucleated followed by vigorous curettage of the surgical margins. None treatment was proposed for the lesions in mandible, except for appropriate information to the patient about the nature of the lesion. Radiographic follow-up was warranted and the patient did not present recurrence four years after treatment.
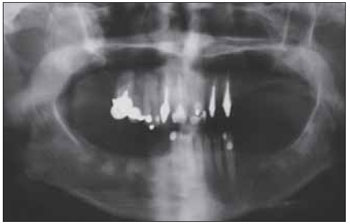 Figure 1. Panoramic Radiographic. - Panoramic Radiographic showing a well defined 4cm unilocular radiopaque defect effacing the right maxillary sinus and sclerotic masses with mixed density in premolar and molar regions of the mandible in the right side.
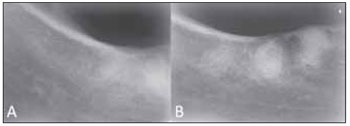 Figure 2. Periapical radiographics of the right mandible.
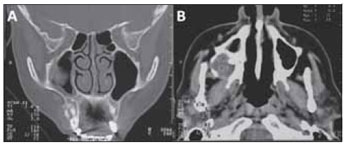 Figure 3. Axial and coronal computerized tomography delineated an hypodense spherical lesion in the right maxilla.
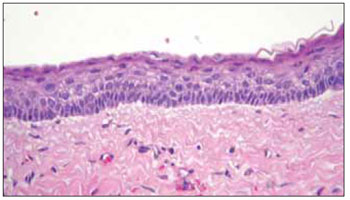 Figure 4. Microscopical diagnosis - Section stained with hematoxin and eosin showing cystic lining with parakeratinized stratified squamous epithelium.
DISCUSSION
Classic radiograph aspect comprises a radiolucent lesion with well defined borders. Most common sites of occurrence are mandibular third molar and ramus region, followed by anterior maxilla, maxillary third molar area, mandibular anterior, and mandibular premolar areas (5,9). Overall maxillary involvement has been observed in ranges from 16.4% (7) to 23.5% (5) of KOT and one percent of the lesions occur in the maxilla with sinus involvement (9). In the latter instance, an apparent radiopaque alteration may be found, differing from the classic description for this lesion. Such aspect has been reported by previous authors to resemble inflammatory antral pseudocyst, which is frequently associated to relevant symptoms, an important clue to differentiate it from other lesions. In addition, computerized tomography imaging of the present case depicted a thin rim of bone surrounding the lesion, as previously reported for KOT (10).
The radiopaque aspect is probably due to increased density of the cystic content in relation to the usual air filling of the sinus. Destruction of sinus floor and walls has also been described for other KOT involving the sinus (11,12), differently from the expansive growth seen the present case. Association in the same patient of KOT with the benign fibro-osseous lesions was probably a coincidence, since we were unable to find out other similar cases in the literature.
Molecular approaches of KOT has been the subject of several studies. Point mutations in the patched (PTCH) tumor suppressor gene have been reported for both the sporadic or nevoid basal cell carcinoma syndrome (13,14). Also, the most substantially over-expressed gene in this lesion is cytokeratin 6B, inferred as cytoskeletal response to increased proliferation of epithelial cells (15). Other over-expressed genes found include epidermal growth factor receptor 3 and glioma-associated oncogene homologue 1 (16). In addition, disruption of fragile histidine triad (FHIT) and p53 genes were detected in many KOT, suggesting participation in the pathogenesis of the lesion, probably due to alteration in proliferative and apoptotic pathways (17). However, specific role in KOT remains controversial (18).
Usual treatment of KOT consist in enucleation, marsupalization, or resection (19). Age of the patient, localization and size of the lesion must be considered in the treatment planning. Anyway, enucleation is the most performed treatment (20), as in the present case.
FINAL COMMENTS
In conclusion, a rare presentation of KOT is described, calling the attention of health care professionals for biologic, diagnostic and therapeutic features of this lesion.
BIBLIOGRAPHICAL REFERENCES
1. Shear M, Speight PM, editors. Cysts of the oral and maxillofacial regions. Oxford: Blackwell; 2007. p. 6-59.
2. Philipsen HP. Keratocystic odontogenic tumour. In: Barnes L, Eveson, JW, Reichart P, Sidransky D, editors. World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005. p. 306-7.
3. Ide F, Obara K, Yamada H, Mishima K, Saito I, Horie N, Shimoyama T, Kusama K. Hamartomatous proliferatinons of odontogenic epithelium within the jaws: a potential histogenic source of intraosseous epithelial odontogenic tumors. J Oral Pathol Med. 2007, 36(4):229-35.
4. Gomez RS, De Marco L. Possible molecular approach to the treatment of odontogenic keratocyst. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005, 99(5):527-8.
5. Myoung H, Hong SP, Hong SD, Lee JI, Lim CY, Choung PH, Lee JH, Choi JY, Seo BM, Kim MJ. Odontogenic keratocyst: Review of 256 cases for recurrence and clinicopathologic parameters. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001, 91(3):328-33.
6. Press SG. Odontogenic tumors of the maxillary sinus. Curr Opin Otolaryngol Head Neck Surg. 2008, 16(1):47-54.
7. González-Alva P, Tanaka A, Oku Y, Yoshizawa D, Itoh S, Sakashita H, Ide F, Tajima Y, Kusama K. Keratocystic odontogenic tumor: a retrospective study of 183 cases. J Oral Sci. 2008, 50(2):205-12.
8. Regezi JA. Odontogenic cysts, odontogenic tumors, fibroosseous, and giant cell lesions of the jaws. Mod Pathol. 2002, 15(3):331-41.
9. Brannon RB. The odontogenic keratocyst. A clinico pathologic study of 312 cases. Part I. Clinical features. Oral Surg Oral Med Oral Pathol. 1976, 42(1):54-72.
10. Damm DD. Dome-like radiodensity of the maxillary sinus. Odontogenic keratocyst. Gen Dent. 2008, 56(7):761-63.
11. Absi EG, Sim RL. Odontogenic keratocyst involving the maxillary sinus: report of two cases. Dentomaxillofac Radiol. 1994, 23(4):226-9.
12. Vencio EF, Mota A, de Melo Pinho C, Dias Filho AA. Odontogenic keratocyst in maxillary sinus with invasive behaviour. J Oral Pathol Med. 2006, 35(4):249-51.
13. Barreto DC, Gomez RS, Bale AE, Boson WL, De Marco L. PTCH gene mutations in odontogenic keratocysts. J Dent Res. 2000, 79(6):1418-22.
14. Sun LS, Li XF, Li TJ. PTCH1 and SMO gene alterations in keratocystic odontogenic tumors. J Dent Res. 2008, 87(6):575-9.
15. Rogers MA, Edler L, Winter H, Langbein L, Beckmann I, Schweizer J. Characterization of new members of the human type II keratin gene family and a general evaluation of the keratin gene domain on chromosome 12q13.13. J Invest Dermatol. 2005, 124(3):536-44.
16. Heikinheimo K, Jee KJ, Morgan PR, Nagy B, Knuutila S, Leivo I. Genetic changes in sporadic keratocystic odontogenic tumors (odontogenic keratocysts). J Dent Res. 2007, 86(6):544-9.
17. Malciæ A, Jukiæ S, Aniæ I, Paveliæ B, Kapitanoviæ S, Kruslin B, Paveliæ K. Alterations of FHIT and P53 genes in keratocystic odontogenic tumor, dentigerous and radicular cyst. J Oral Pathol Med. 2008, 37(5):294-301.
18. González-Moles MA, Mosqueda-Taylor A, Delgado-Rodríguez M, Martínez-Mata G, Gil-Montoya JA, Díaz-Franco MA, Bravo-Pérez JJ, M-González N. Analysis of p53 protein by PAb240, Ki-67 expression and human papillomavirus DNA detection in different types of odontogenic keratocyst. Anticancer Res. 2006, 26(1A):175-81.
19. Bsoul SA, Paquette M, Terezhalmy GT, Moore WS. Odontogenic keratocyst. Quintessence Int. 2002, 33(5):400-1.
20. Morgan TA, Burton CC, Qian F. A retrospective review of treatment of the odontogenic keratocyst. J Oral Maxillofac Surg. 2005, 63(5):635-9.
1 Master of Dentistry. MSc Faculty of Dentistry, Federal University of Uberlandia.
2 Specialist. Expertise in Oral and Maxillofacial Surgery-Maxillo-Facial Surgery, Faculty of Dentistry, Federal University of Uberlandia.
3 Doctor. Associate Professor, Department of Oral and Maxillofacial Surgery-Maxillo-Facial Surgery, Faculty of Dentistry, Federal University of Uberlandia.
4 Doctor. Associate Professor, Department of Oral Pathology, School of Dentistry, Federal University of Uberlandia.
5 Doctor. Professor, Department of Oral Pathology, School of Dentistry, Federal University of Uberlandia.
6 Doctor. Professor, Department of Stomatology, School of Dentistry, Federal University of Uberlandia.
Institution: Universidade Federal de Uberlândia. Uberlândia / MG - Brazil. Mail address: Gustavo Davi Rabelo - Alameda Himalaia, 341 - Bairro Mansões Aeroporto - Uberlândia / MG - Brazil - Zip code: 38406-389 - Fax and Telephone: (+55 34) 3211-3690 - E-mail: drgustavorabelo@yahoo.com.br
Article received March 27, 2009. Article approvad April 28, 2009.
|
|
 |
|
|
