|
809 |
|
Year: 2011 Vol. 15 Num. 4 - Out/Dez - (10º)
DOI: 10.1590/S1809-48722011000400010
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Characteristics of the tinnitus and hyperacusis in normal hearing individuals |
|
| Author(s): |
| Daila Urnau1, Tania Maria Tochetto2.
|
|
|
| Key words: |
| hearing, tinnitus, hyperacusis, questionnaires. |
|
|
 |
| Abstract: |
Introduction: The tinnitus has become a common otological complaint. Another complaint is found in bearers of the tinnitus is the hyperacusis. Objective: Analyze the characteristics of tinnitus and hyperacusis in normal hearing individuals with associated complaints of tinnitus and hyperacusis. Method: 25 normal hearing individuals who complained of hyperacusis and tinnitus were surveyed in this form of cross-sectional study. They were questioned about the location and type of the tinnitus. The evaluation of the tinnitus was made using the Brazilian Tinnitus Handicap Inventory and acuphenometry. A questionnaire was made about the hyperacusis covering aspects such as: sounds considered uncomfortable, sensations in the presence of such sounds, and difficulty understanding speech in noise. Results: Of the 25 individuals, 64% were women and 36% men. Regarding tinnitus, 84% referred to bilateral location and 80% high pitch. The most common degree found was light (44%). The women presented tinnitus degree statistically superior to those of men. The strong intensity sounds and the reactions of irritation, anxiety and the need to move away from the sound were the most mentioned. From the analyzed individuals, 68% referred to difficulty understanding speech in noise and 12% reported using hearing protection. The most found frequencies at the acuphenometry were 6 and 8 KHz. Conclusion: Normal hearing individuals who complain of tinnitus and hyperacusis present mainly high pitch tinnitus, located bilaterally and light degree. The sounds considered uncomfortable were the high intensity ones and the most cited reaction to sound was irritation. The difficulty to understand speech in noise was reported by most of the individuals.
|
|
|
INTRODUCTION
The tinnitus has become a common otological complaint. It is estimated that approximately 25 million Brazilians present such symptom (1).
A complete anamnesis about the installation of the symptom, description, localization, nuisance caused, among others, is the first action in face of individuals complaining of tinnitus (2). The use of questionnaires is of great value for the assessment of the presence and determination of the degree of severity of the tinnitus (3).
One of the oldest methods still in use to assess the tinnitus is the Acuphenometry (4).
The Tinnitus Handicap Inventory (THI) is a questionnaire that seeks to characterize and identify the tinnitus. It is succinct, of easy application and interpretation and reliability for the clinical practice. It addresses the interference of the tinnitus on the patient's quality of life: functional, emotional and catastrophic reactions to tinnitus (5). The THI was translated and validated to Brazilian Portuguese in 2005 by FERREIRA et al (6).
Another complaint that has been found in bearers of tinnitus is the hyperacusis (7, 8, 9, 10). The hyperacusis is a tolerance reaction to environmental sounds, an exaggerated or inappropriate response to sounds that do not cause nuisance to the general population. Its prevalence varies from 9 to 15%, but this percentage is higher in people who present tinnitus (8).
The decrease of noise tolerance is present when the individual reacts negatively to the presence of a sound that would not evoke similar reactions in normal hearers. Such reactions can be of discomfort, fear, nuisance, suffering and others (11). The authors compare the reaction of discomfort of people with hyperacusis (usually for weak sounds) to the reaction of normal individuals in the presence of a high intensity sound.
The hyperacusis occurs in individuals with normal hearing (12, 7). Of the individuals with complaints of tinnitus, only 8 to 20% present normal hearing (13, 12, 7).
METHOD
This is a cross-sectional, descriptive, non-experimental, quantitative study of data obtained from normal hearing volunteers who complained of hyperacusis and tinnitus. To recruit subjects, the research was announced on the site of Universidade Federal de Santa Maria (UFSM), local papers and radio stations.
The data collection occurred from May to July of 2010, at the Speech-Therapy Service (STS) of UFSM. Participated on the research only individuals who agreed with the methodology of the study, signing the Term of Free and Informed Consent (following Resolution 196/1996).
This study was attached to the Project "Research and database in auditory health", registered at the Ethics in Research Committee, under the number 0138.0.243.246-06.
Through anamnesis was investigated the existence of tinnitus and hyperacusis. Also, it was researched the location (unilateral or bilateral) and the type of tinnitus (if bass or treble). Were included on the study only normal hearing individuals who presented complaints of hyperacusis and tinnitus.
Were considered normal hearing individuals only those that, on the Pure Tone Audiometry, showed air thresholds not above 25 dB in every frequency (14), tympanogram type A (15) and presence of acoustic reflexes.
A visual inspection of the external auditory canal was conducted to discard the presence of obstacles to the realization of PTA. That was performed by air at frequencies of 250, 500, 1000, 2000, 3000, 4000, 6000 and 8000 Hz and through bone transmission at frequencies of 500, 1000, 2000, 3000 and 4000 Hz. The equipment used was the two channel digital audiometer, brand Fonix, model FA-12, type 1 and earphones type TDH-39P, brand Telephonics.
The tympanometry and the the study of acoustic reflex were determined with the middle ear analyzer of the brand Interacoustics AZ7, with phone TDH-39 and pad MX-41, with probe-tone of 220 Hz at 70 dB NA for tympanometry, and calibration following the norm ISO 389-1991.
The sample consisted of 25 individuals, with ages from 21 to 70 years, being 16 females and 9 males.
To assess the tinnitus was used the Brazilian THI (6). After completed, the points were summed, classifying the tinnitus in degrees: slight, mild, moderate, severe and catastrophic (16).
For the analysis and characterization of hyperacusis, a questionnaire was developed, based on publication by Aita (7) and GONÇALVES, TOCHETTO and GAMBINI (17). The questionnaire addressed aspects such as: sounds considered uncomfortable (police siren, bell, slamming door, music in normal and loud volume, etc.), difficulty to understand speech in noise, situations that cause discomfort, sensations on the presence of uncomfortable sounds (fear, tension, annoyance, necessity to go away from the sound, tinnitus, etc), use of ear plugs and for how long tolerates these sounds (less than 1 minute, from 1 to 5, from 5 to 10, or more than 10 minutes).
The individuals underwent acuphenometry. In this study, only the pitch (sensation of sound frequency) of the tinnitus was researched. According to the type of tinnitus reported by the patient, it was presented a pure tone ore a narrow band noise, or else a broadband noise (white noise), to the ear contralateral to the tinnitus, thus determining its pitch.
In order to verify if there was compatibility between the pitch reported by the patient and the one found in acuphenometry, the narrow band noise and the pure tone above 1 KHz were classified as treble pitch and below 1KHz as bass. The broadband noise, once covers a wide range of frequencies, was considered to be compatible with either reported pich, treble or bass.
The data were tabled and analyzed descriptively and statistically using the U test of Mann-Whitney and Kruskal-Wallis test. The degree of significance adopted was 5% (p<0.05).
RESULTS
The analyzed sample consisted of 64% female and 36% male individuals.
From the 25 analyzed individuals, the most common location of the tinnitus was bilateral (84%). Of the 16% who reported unilateral tinnitus, the right ear was predominant (75%) over the left ear (25%). Concerning the pitch of the tinnitus, 80% of the individuals reported it as treble.
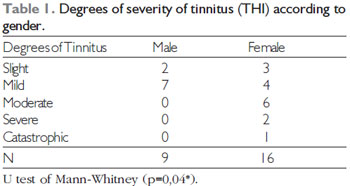
The results of the degree of tinnitus according to the THI, considering the totality of the subjects studied, are shown in Figure 1. The distribution of degrees of tinnitus in relation to gender is in Table 1.
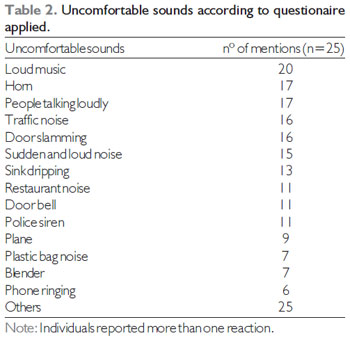
Table 2 shows the sounds considered uncomfortable, according to the hyperacusis questionnaire.
We considered "other sounds" those with less than five mentions: car started (4), loud laughter (3), fridge noise (3), sound of music at regular volume (2), motorcycle noise (2), alarm clock (2), clapping (1), key noises (1), repetitive noises (1), crying child (1), shower noise (1), television at regular volume (1), tableware scraping on the plate (1), rockets (1) and microphone interference (1).
Still regarding the hyperacusis questionnaire used, 68% of the individuals reported difficulty in understanding speech in noise. Regarding the situations that cause discomfort, eight answers were obtained. The absence of situations that elicit the discomfort was the most mentioned, followed by "at the end of the day" and "when I'm stressed".
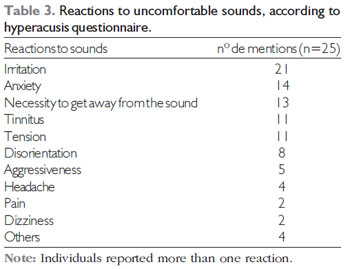
Table 3 shows the reactions to uncomfortable sounds, according to the hyperacusis questionnaire.
In Table 3, "other reactions"were those with only one mention each: shock, a wish to cry, fear and panic.
As for the use of earplugs, 88% reported not to use them. There was a predominance of 5 to 10 minutes of tolerance time to the sounds considered uncomfortable.
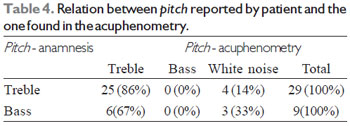
The frequencies most commonly found in the acuphenometry were the treble, especially 6 and 8 KHz. Table 4 shows the results of the analysis by ear, between the referred pitch at anamnesis and the one found in the acuphenometry. It was not possible to apply statistical tests on these findings.
Nine subjects reported tinnitus of bass pitch, though such finding was not verified by acuphenometry. That is to say that this individuals identified a treble sound (pure tone or narrow band noise) or white noise instead of the referred bass.
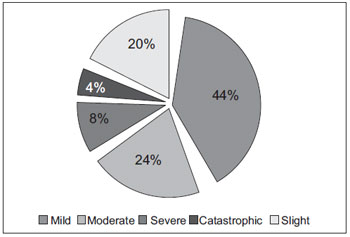 Figure 1. Distribution of the degrees of severity of tinnitus according to THI in all evaluated individuals.
DISCUSSION
The assossiation between tinnitus and hyperacusis is frequently found in literature: 63% (8, 10), 66,7% (7) and 90% (9). However, we did not find studies that investigate subjects with these two concomitant complaints. Therefore, the obtained data were compared to studies made only with people with hyperacusis and only with bearers of tinnitus.
This study found greater representation of female individuals (64%). Women are more affected both by hyperacusis (61%) (8), and by tinnitus (67,3%) (18), (52,1%).
However, there is controversy in literature about the influence of gender in the prevalence of tinnitus (19). We believe that the higher percentage of women found is due to the fact that they are more available to seek medical care (20), since the female gender prevails in the search for health services (21).
It was observed the prevalence of subjects afflicted by tinnitus of bilateral location (84%). Similar findings, though with smaller percentages, were found by other studies (17, 19). For their turn, FERNANDES and SANTOS (22) found only 20% of the sample reporting bilateral tinnitus.
In this study, the unilateral affection of the right ear was more reported than the left. The study of MARTINES et al. (23) goes to meet this finding. But in article by FERNANDEZ and SANTOS (22), the unilateral affection of the left ear was the most common (65%).
The most found pitch, both in anamnesis as in acuphenometry (Table 4), was the treble, especially at frequencies of 6 and 8 KHz. Literature also shows treble pitch tinnitus as the most reported by patients with tinnitus (22, 23, 24). As in this study, MENEZES and SANTOS FILHA (4) relate higher occurrence of treble tinnitus at the same frequencies.
The most commom degree of tinnitus was mild (44%) (Figure 1), which agrees with the findings of MARTINES et al. (23) and PAGLIALONGA et al. (25), because they found the same degree in normal hearing individuals. On the other hand, PINTO, SANCHEZ & TOMITA (19) obtained higher percentage of the slight degree and SAVASTANO (26) of the moderate degree, using the same assessment instrument. The low scores found can be explained, since in about 80% of the cases the tinnitus does not cause discomfort for the patient (1, 27).
SAVASTANO (26) found association of slight and mild degrees of tinnitus to individuals who had hearing loss, and moderate to catastrophic degrees associated to individuals without hearing loss, which was not verified in this study. According to this author, a greater degree of hearing loss does not correlate to greater nuisance with the tinnitus.
According to THI, the degree of tinnitus was statistically higher in women (Table 1). This finding can be explained by the greater prevalence of affective disorders, such as anxiety and depression, in women (19), since they are frequently described and associated to a greater nuisance to tinnitus (28).
On the contrary, PINTO, SANCHEZ & TOMITA (19) did not find statistically significant correlation between gender and the nuisance caused by tinnitus, according to THI. These authors refer to depression as a possible indirect influence of gender, showing incidence twice as high in females as in males (29).
The high intensity sounds were the uncomfortable sounds most mentioned by the individuals: high volume music sounds, horn, people talking loudly, traffic noise, door slamming, sudden and high sound, in this order (Table 2).
In study performed with musicians with hyperacusis, GONÇALVES, TOCHETTO & GAMBINI (17) also found, mainly, the high intensity souns to be discomforting: traffic noise, door slamming, and high volume music. The sounds that started hyperacusis, in AITA's study (7), were: music, sounds of planes and motors in general. Sounds of telephone, doorbell, sirens and slamming doors were also mentioned, but less frequently.
The difficulty to understand speech in noise mentioned (68%) may be deeply connected to the mechanism of tinnitus and hyperacusis, through the Olivocochlear Medial System (OMS); this system acts as a modulator to the activity of the external ciliated cells (ECC) of the cochlea and, among other functions, acts in the recognition of auditory stimuli in the presence of competitive noise (12).
We believe that in, people afflicted by tinnitus, occurs a loss of modulation of the ECC, causing an abnormal auditory pathways activity, misinterpreted as a sound. In hyperacusis, the ECC cease to perform their function of non-linear amplification, beginning to amplify low and moderat intensity sounds (30). Probably, a cortico-thalamic-olivary pathway is responsible for selective attention and cochlear modulation, both important in the discrimination of speech in the presence of noise (12).
Thus, a disorder of the OMS might cause the tinnitus, hyperacusis and difficulty to recognize speech in noise, as demonstrated by HENNING et al. (31). In the mentioned study, normal hearing individuals with complaints of tinnitus and hyperacusis showed lower performance in the presence of noise, with statistically significant difference, when compared to normal hearing individuals without auditory complaints.
The most common reactions to sound were irritation, anxiety, necessity to get away from the sound, tinnitus, tension and disorientation (Table 3). AITA (7) found similar reactions: irritation, tinnitus, headache, hearing decrease, aggressiveness, nausea and anguish. GONÇALVES, TOCHETTO & GAMBINI (17), on the other hand, reported tension, anxiety, necessity to get away from the sound, anger, irritation and pain, being similar to this study, only with different number of mentions.
Hypersensitivity can cause anxiety and even fear, occurring for specific sounds as well as general sounds. This happens because the connections between the central auditory system and the brain areas involved in anxiety and fear are closely connected (32).
Due to these reactions caused by uncomfortable sounds, 12% of the researched individuals reported the use o earplugs. VALENTE et al. (33) found constant use of earplugs in severe cases of hyperacusis, because even conversation caused nuisance. According to BAGULEY (32) the first reaction to the hyperacusis is to protect oneself with earplugs or other such devices.
It is noteworthy that auditory overprotection is contraindicated, because it can raise even more the central hearing gain and aggravate the hyperacusis (32). In fact, the Tinnitus Retraining Therapy, sound therapy indicated to tinnitus and hyperacusis, is based on auditory desensitization, which involves the gradual removal of earplugs (34).
Most of the subjects questioned reported 5 to 10 minutes of tolerance to sounds considered uncomfortable. AITA (7) found time lower than one houre.
In the acuphenometry (Table 4), the bass pitch reported by some subjects was not confirmed. Adding to the results found, MOR (35) also found in acuphenometry prevalence of treble pitch, especially at frequencies of 6 to 8 KHz, in normal hearing individuals with complaints of tinnitus.
The absence of relation between the pitch reported in the anamnesis and the one found in the acuphenometry may have occurred due to patient's difficulty to compare and associate pure tones or noises to tinnitus, apart from tinnitus being multitonal, in most cases (24).
CONCLUSION
Normal hearing individuals with complaints of tinnitus and hyperacusis show prevalence of treble pitch tinnitus, located bilaterally and of mild degree. The degree of tinnitus was more accentuated on females.
The high intensity sounds were considered the most uncomfortable. The most mentioned reactions to these sounds were: irritation, anxiety and necessity to get away from the sound. The difficulty to understand speech in the presence of noise was reported by most of the individuals
BIBLIOGRAPHIC REFERENCES
1. Sanchez TG, Ferrari GMS. O que é zumbido? Em: Samelli AG. Zumbido: avaliação, diagnóstico e reabilitação: abordagens atuais. São Paulo: Lovise; 2004. p. 17-22.
2. Branco-Barreiro FCA. Avaliação audiológica básica e psicoacústica do zumbido. Em: Samelli AG. Zumbido: avaliação, diagnóstico e reabilitação: abordagens atuais. São Paulo: Lovise; 2004. p.55-60.
3. Jastreboff MM, Jastreboff PJ. Questionnaires for Assessment of the Patients and Treatment Outcome. Em: Hazel JWP (ed). Prodeeding of the IV International Seminar.Cambridge (UK); 1999. p.487.
4. Menezes P, Santos Filha VAV. Acufenometria: o resgate de um instrumento de avaliação do zumbido e sua correlação com perdas auditivas sensoriais. Fonoaudiologia Brasil. 2005, 3(1):1-4.
5. Newman C, Jacobson CG, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1996, 122(2):143-148.
6. Ferreira PEA, Cunha F, Onishi ET, Branco-Barreiro FCA, Ganança FF. Tinnitus Handicap Inventory: adaptação cultural para o português brasileiro. Pró-Fono. 2005, 3(17):303-10.
7. Aita ALD. Capacidade e auto-percepção auditivas: um estudo em hiperacúsicos. São Paulo; 2001.(Tese de Doutorado em Distúrbios da Comunicação Humana: Campo Fonoaudiológico, Universidade Federal de São Paulo).
8. Herráiz C, Hernández JC, Plaza G, Toledano A, de los Santos G. Estudio de la hiperacusia en una unidad de acúfenos. Acta Otorrinolaringol Esp. 2003, 54(9):617-622.
9. Herráiz C, de los Santos G, Diges I, Díez R, Aparicio JM. Evaluación de la hiperacusia: test de hipersensibilidad al sonido. Acta Otorrinolaringol Esp. 2006, 57(7):303-306.
10. Sztuka A, Po[piech L, Gawron W, Dudek K. DPOAE in estimation of the function of the cochlea in tinnitus patients with normal hearing. Auris Nasus Larynx. 2010, 37(1):55-60.
11. Jastreboff PJ, Jastreboff MM. Decreased sound tolerante. Em: Snow, J.B. (ed) Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker Inc, 2004, p. 8-15.
12. Breuel MLF, Sanchez TZ, Bento RF. Vias auditivas eferentes e seu papel no sistema auditivo. Arq Otorrinolaringol. 2001, 5(2):62-7.
13. Jastreboff PJ, Hazell, JWP. A neurophysiological approach to tinnitus: clinical implications. Br J Audiol. 1993, 27(1):7-17.
14. Lloyd LL, Kaplan H. Audiometric interpretation: a manual o basic audiometry. University Park Press: Baltimore; 1978. p. 16-7.
15. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryng. 1970, 92(4):311-24.
16. Figueiredo RR, Azevedo AA, Oliveira PA. Análise da correlação entre a escala visual-análoga e o Tinnitus Handicap Inventory na avaliação de pacientes com zumbido. Rev Bras Otorrinolaringol. 2009, 75(1):76-9.
17. Gonçalves MS, Tochetto TM, Gambini C. Hiperacusia em músicos de banda militar. Rev Soc Bras Fonoaudiol. 2007, 12(4):298-303.
18. Sanchez TG, Medeiros IRT, Levy CPD, Ramalho JRO, Bento RF. Zumbido em pacientes com audiometria normal: caracterização clínica e repercussões. Rev Bras Otorrinolaringol. 2005, 71(4):427-431
19. Pinto PCL, Sanchez TG, Tomita S. Avaliação da relação entre severidade do zumbido e perda auditiva, sexo e idade do paciente. Braz J Otorhinolaryngol. 2010, 76(1):18-24.
20. Coelho CB, Sanchez TG, Ferreira Bento RF. Características do zumbido em pacientes atendidos em serviço de referência. Arq Inter Otorrinolaringol. 2004, 8(3):284-91.
21. Pinheiro RS, Viacava F, Travassos C, Brito AS. Gênero, morbidade, acesso e utilização de serviços de saúde no Brasil. Ciênc. Saúde Coletiva. 2002, 7(4):687-7070.
22. Fernandes LC, Santos TMM. Zumbido e audição normal: estudo da supressão das emissões otoacústicas transientes. Braz J Otorhinolaryngol. 2009, 75(3):414-9.
23. Martines F, Bentivegna D, Martines E, Sciacca V, Martinciglio G. Assessing audiological, pathophysiological and psychological variables in tinnitus patients with or without hearing loss. Eur Arch Otorhinolaryngol. 2010, 267(11):1685-1693.
24. Azevedo AA, Mello PO, Siqueira AG, Figueiredo RR. Análise Crítica dos Métodos de Mensuração do zumbido. Rev Bras Otorrinolaringol. 2007, 73(3):418-23.
25. Paglialonga A, Del Bo L, Ravazzani P, Tognola G.Quantitative analysis of cochlear active mechanisms in tinnitus subjects with normal hearing sensitivity: multiparametric recording of evoked otoacoustic emissions and contralateral suppression. Auris Nasus Larynx. 2010, 37(3):291-298.
26. Savastano, M. Tinnitus with and without hearing loss: are its characteristics different? Eur Arch Otorhinolaryngol. 2004, 265(11):1295-300.
27. Fukuda Y. Zumbido Neurossensorial. Rev Neurociências. 2000, 8(1):6-10.
28. Londero A, Peignard P, Malinvaud D, Avan P, Bonfils P.Tinnitus and cognitive-behavioral therapy: Results after one year. Presse Med. 2006, 35(9):1213-21.
29. Dobie RA, Sullivan MD. Antidepressant drugs and tinnitus. Em: Vernon JA. Tinnitus Treatment and Relie. Boston: Allyn and Bacon; 1998. p. 43-51.
30. Jastreboff PJ. Phantom auditory perception (Tinnitus). Mechanisms of generation and perception. Neurosci Res. 1990, 8(4):221-54.
31. Hennig TR, Costa MJ, Urnau D, Becker KT, Schuster LC. Reconhecimento de fala de indivíduos normo-ouvintes com zumbido e hiperacusia. Arq Inter Otorrinolaringol. 2011, 15(1):21-8.
32. Baguley DM. Hyperacusis. J R Soc Med. 2003, 96(12):582-5.
33. Valente M, Goebel J, Duddy D, Sinks B, Peterein J. Evaluation and treatment of severe hyperacusis. J Am Acad Audiol. 2000, 11(6):295- 299.
34. Jastreboff PJ, Jastreboff MM. Tinnitus Retrainning Therapy (TRT) as a method of tinnitus and hiperacusis patients. J Am Acad Audiol. 2000, 11(3):162-167.
35. MOR R. Emissões otoacústicas e audiometria de altas frequências: estudo em pacientes com zumbido sem perda auditiva. São Paulo, 2003 (Dissertação de Mestrado- UNIFESP).
1) Post graduate. Speech Therapist.
2) Doctor in Science of Human Communication Disorders. Professor Associate to the Departament of Phonoaudiology of UFSM, Santa Maria (RS), Brazil.
Institution: Federal University of Santa Maria. Santa Maria / RS - Brazil. Mailling address: Street Lava Pés, 878 - Apartment 103 - Downtown - Passo Fundo / RS - Brazil - ZIP code: 99010-170 Telephone: (+5554) 91355594 - E-mail: daila_urnau@yahoo.com.br
Article received in March 28 of 2011. Article approved in July 10th of 2011.
|
|
 |
|
|