INTRODUCTIONThe Bone anchored hearing aid is a favorable means of providing hearing rehabilitation to certain group of patients like patients with aural atresia and severe conductive hearing loss (1). In these patients, conventional hearing aid cannot be used. The system utilizes Brånemark System® implants in combination with a bone anchored sound processor. The long-term success of such system is based on the active bond between the bone and the implant at the molecular level (2) (osseointegration). The true bone conducted sound without the interposition of soft tissues that attenuate the sound signal gives excellent quality of hearing to the patient.
CASE REPORT A seven year old male child from Kathmandu, Nepal was brought by his parents to the ENT Outpatient department of TU Teaching Hospital with history of congenital absence of bilateral pinna, nonprogressive bilateral hearing loss and delayed speech. Apart from these abnormalities the patient had a normal perinatal history. There was no history of major illnesses in the past. No similar history was present in the family members.
On examination, the child had absence of bilateral pinna. The tuning fork test was difficult to perform. The facial nerve was intact. His speech was unclear though he could follow the commands correctly. Rest of the ENT and Head & Surgery examination and the systemic examination was normal.
On investigation, his hemoglobin was 11.2 gm%. Routine blood count was normal. Pure tone audiometry showed bilateral conductive hearing loss with an average of 60dB air bone gap. The aided threshold showed improvement bilaterally with an average of 38dB air bone gap. The CT scan of the temporal bone showed absence of the pinna bilaterally with normal middle and inner ear structures. The mastoid bone was thicker in the right side as compared to the left.
The surgery was performed under general anesthesia. The patient was planned for the insertion of the BAHA on the right side since the mastoid bone was thick on that side compared to the left making it easier for the insertion of the implant, as per the CT scan finding. After the postaural skin incision, the implant site was prepared using a guide drill in the mastoid bone. The bone thickness drilled was 2.8 mm. The implant was then inserted in the mastoid bone. The second implant was inserted 1.5 cm posterior to the first implant. Thus, the first stage of the operation was completed and the flap was closed. The second stage of the operation was planned after 6 months. The postoperative period was uneventful. The child was sent home on the 4th postoperative day. The stitches were removed on the 6th postoperative day with no postoperative complications till date.

Fig.1. CT Scan showing bilateral absence of pinna and external auditory canal.
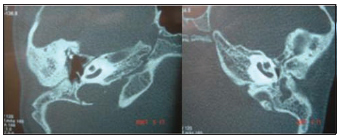
Fig.2. CT Scan showing bilateral normal middle ear volume and normal inner ear.

Fig. 3. Postoperative photo of the patient showing sutured site.
The Conventional hearing aid consists of an electromagnetic vibrator pressed against the mastoid process held by steel sprung and connected to a body worn processor. The pressure required to press the transducer to the mastoid for sound transmission cause discomfort to the patient (1,3). This led to the development of newer technologies like the Xomed Audiant bone conductor and the Bone Anchored hearing aid (BAHA) (1).
The development of BAHA led to the hearing rehabilitation of patients like aural atresia and chronically discharging ears. Brånemark was the first person to discover the unique property of titanium to get firmly attached to the bone without any reaction at the implant-bone interface (osseointegration). The BAHA gives the true bone conducted sound, without the intervening soft tissue that distort the signal, giving better quality of sound. Here, there is a microphone connected to a titanium-coupling device attached to the titanium fixture. Coupling the bone vibrator to an osseointegrated implant gives better quality of sound, better cosmetic advantage and binaural hearing. The only disadvantage is its cost.
The BAHA surgery is usually done as a single stage operation where the titanium fixture and the abutment are done in a single stage. In some cases the operation is done in two stages like in the case we have reported. Here, the titanium fixture is placed in the first stage and the abutment is done in the second stage usually after 6 months though the duration can vary from seven to eight months (4). This is done in children where the mastoid bone is thin or irradiated patient where there is poor bone quality. The average of six month is given for the osseointegration of the fixture with the mastoid bone.
Though there is no fixed age for the BAHA surgery, DRINIAS et al. (5) mentioned the better chance of osseointegration in children due to better blood flow in the temporal bone as compared to the elderly. Two fixtures were kept on this reported case since that reduces the duration of disability in case one fixture fails. Additionally, the fixture with the better osseointegration can be used for the placement of abutment (6).LLOYD et al. (7) mentioned the experiences of BAHA in children in 85 ears. They had suggested that BAHA provide significant benefit over the other types of hearing aid both audiologically and in terms of quality of life. Careful selection of candidates and methodical followup are required which is also supported by YELLON et al. (3).
CONCLUSIONBone anchored hearing aid is a favorable means of providing hearing rehabilitation to certain group of patients like patients with aural atresia and severe conductive hearing loss. It provides benefit over the other types of hearing aid both audiologically and in terms of quality of life. We are reporting this case, as this is the first bone anchored hearing aid surgery done in Nepal.
REFERENCES1. Proops DW. Surgery of congenital abnormalities of external and middle ears. Scott-Brown's Otolaryngology. 6th edition. Reed Educational and Professional Publishing Ltd. 1997, 6/9/10-6/9/12.
2. Santina CCD, Lustig LR. Surgically implantable hearing aids. Cummings Otolaryngology Head & Neck Surgery. 4th edition. Elsevier Mosby, Philadelphia, USA. 2005; 3593-7.
3. Siegert R, Mattheis S, Kasic J. Fully implantable hearing aids in patients with congenital auricular atresia. Laryngoscope. 2007, 117:336-40.
4. Davids T, Gordon KA, Clutton D, Papsin BC. Bone - anchored hearing aids in infants and children younger than 5 years. Arch Otolaryngol Head Neck Surg. 2007, 133:51-5.
5. Drinias V, Granstrom G, Tjellstrom A. High age at the Time of Implant Instillation is correlated with Increased Loss of Osseointegrated Implants in the Temporal Bone. Clin Implant Dent Relat Res. 2007, 9:94-9.
6. Durvasula VS, Patel H, Mahendra S, Gray RF. Bone anchored hearing aids: a second fixture reduces auditory deprivation in Cambridge. Eur Arch Otorhinolaryngol. 2007. April 6:[Epub ahead of print].
7. Lloyd S, Almeyda J, Sirimanna KS, Albert DM, Bailey CM.Updated surgical experience with bone-anchored hearing aids in children. J Laryngol Otol. 2007, 9:1-6.
8. Yellon RF. Bone anchored hearing aid in childrenprevention of complications. Int J Pediatr Otorhinolaryngol. 2007, 71:823-6.
1. Dr. (Teaching Assistant).
2. Dr. (M.S.Third Year Resident).
3. Dr. (M.S. First Year Resident).
4. Dr. (Associate Professor).
5. Prof. (Professor).
Institute: T. U. Teaching Hospital, Maharajgung, Kathmandu, Nepal.
Address for correspondence:
Dr Prakash Adhikari
M.S. First Year Resident, Department of ENT and Head & Neck Surgery
TU Teaching Hospital, Maharajgunj, Kathmandu - Nepal
Tel: 977-01-4414191
Artigo recebido em 18 de agosto de 2007.
Artigo aceito em 8 de novembro de 2007.

