INTRODUCTIONThe severe epistaxis is considered to be the main emergency in the otorhinolaryngologic practice and causes important hospital interment. The root of the problem is multifunctional and results from a number of factors that affect the nasal mucosa and the blood vessels, including environmental, local and systemic factors. According to the original region, the epistaxis is classified as anterior and posterior. In the anterior epistaxis, the blood loss is generally of low volume and does not provoke major complications; but the nasal bleeding should never be underestimated, because it may be the first symptom of an adjacent pathology, such as juvenile nasoangiofibroma, Rendu-Osler-Weber's syndrome (hereditary hemorrhagic telangiectasy) etc., and in such cases, even epistaxis classified as anterior may be severe. In the other hand, the posterior epistaxis is usually more severe. The patient may evolve to a maximum degree of hypovolemic shock and systemic complications. As for the top diagnosis of the severe epistaxis, bleeding may arise from the external or internal carotid artery territory. Approximately 95% of the profuse hemorrhages come from the external carotid branches that are the Sphenopalatine a. and its terminal branches: posterior lateral nasal a. and Nasoseptal a. Only in about 5% of the cases internal Carotid a. territory intense bleeding occurs through its nasal terminal branches: anterior Ethmoidal a. and posterior Ethmoidal a.
In the otorhinolaryngological therapeutic arsenal there are several procedures described to control severe nasal bleeding, which are classified among surgical and nonsurgical. In the past, the surgical procedures were used as alternatives when the conservative treatment failed. However, in the last years, many publications suggest as an initial step for patients with severe epistaxis the surgical control of the sphenopalatine and ethmoidal arteries via endoscopy. Studies have been showing that both ligation and arterial cauterization have efficacy and acceptable cost-benefit ratios for such procedures. In addition, the nasal endoscopic treatment is best tolerated by the patients, since nasal splints result in pain, nasal obstruction and significant morbidity and is not exempted from risk. As for the surgical management complications, we may mention the rates have diminished considerably due to a higher professional experience and deepened knowledge of the nasosinusal endoscopic anatomy.
The endoscopic surgical approach for patients with severe epistaxis is a theme for discussion in the literature. Many approve only the dissection of the sphenopalatine a. pedicles with initial management, due to the major incidence of bleeding from this region. In the other hand, some authors prefer the anterior ethmoidal a. dissection along with the sphenopalatine a. branches, by justifying it with the problem definitive resolution. Those who criticize such approach, do it for several reasons, amongst which the fact that such procedure requires a longer surgical time and causes a large dissection of a generally healthy nasal cavity.
The treatment of the epistaxis from the anterior ethmoidal a. became more effective with the advent of nasal endoscopy techniques. The approach needs suitable instruments and angulated optics to prevent complications, amongst which, liquoric fistula, intraorbitary hemorrhage, lesion of the medial straight m., amaurosis etc. Traditionally, this territory bleeding control was made through Lynch's incision in the medial orbital border and dissection between the periorbital and papyraceous lamina, with connection or cauterization of the anterior ethmoidal artery. The endoscopic approach allows a more precise localization of the bleeding origin and a more effective control.
The objective of this work is to report the experience of the Otorhinolaryngology Service at PUCPR in the endoscopic treatment of the epistaxis resulting from the anterior ethmoidal a.
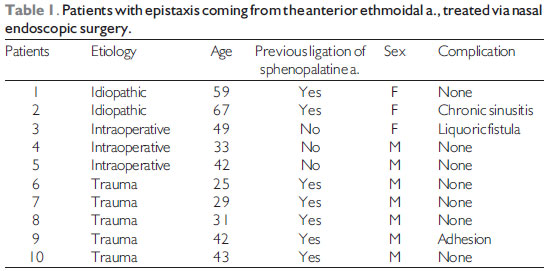
METHODBetween May 2005 and December 2008, 10 patients who presented with anterior ethmoidal a. severe epistaxis were treated with endoscopy. The age ranged from 25 to 67 years and they were 07 men and 03 women. The etiology was varied and is described below: 03 cases resulting from lesion of the artery in the nasal endoscopic surgery intraoperative (30%), 05 cases resulting from face trauma (50%), 02 cases of undetermined etiology (20%). In 07 cases (70%), previous ligation or cauterization of the sphenopalatine a. branches had been carried out with rebleeding in the postoperative and need for cauterization of the ethmoidal a. The diagnosis of all cases was made in the intraoperative through the localization of the anterior ethmoidal artery with active bleeding. The patients who presented bleeding of the nasal cavity roof, but not coming from the anterior ethmoidal artery, whose diagnosis was carried out after its dissection were excluded.
Surgical technique All patients were submitted to the procedure under general intravenous anesthesia, keeping PAM around 60 mmHg; topical hemostasis was made with cottonoid soaked up in a solution of adrenaline and distilled water in the concentration of 1:2000; septoplasty carried out in the necessary cases to facilitate the surgical access; procedure with uncinectomy started, maxillary antrostomy, preserving the ethmoidal bulla, under endoscopic view with optics of 0º; after identification of the ethmoidal bulla, the removal of its upper part is begun under view with optics of 70o (Karl Storz 70º, 4mm); in all cases we observed the anterior ethmoidal artery exposed in the nasal cavity, at approximately 2 cm from the ethmoidal bulla, as the origin of bleeding. in all cases we performed its cauterization through bipolar cautery. RESULTSAll patients evolved without rebleeding after cauterization of the anterior ethmoidal a. In 01 case there was the formation of the iatrogenic liquoric fistula with immediate correction in the intraoperative with satisfactory evolution. In 01 case there was cauterization of the posterior ethmoidal a. due to diagnostic doubt upon surgery. The interment duration ranged from 02 to 07 days. In the postoperative the patients were followed up in the 7th, 14th, 21st, 30th and 60th days. There was 01 case of nasal adhesion and 01 case of chronic sinusitis in the postoperative, which were treated and evolved satisfactorily (Table 1).
DISCUSSIONThe endoscopic surgical approach for patients with severe epistaxis is a theme for discussion in the literature. The severe epistaxis localized in the anterior ethmoidal a. territory is an uncommon event that affects approximately 5% to 18% of the cases of profuse bleeding, and is mostly original from the sphenopalatine a. Many approve only the dissection of pedicles of the sphenopalatine a. as initial management, due to the major incidence of bleeding coming from this region. In the other hand, some authors prefer the anterior ethmoidal a. dissection along with the sphenopalatine a. branches, by justifying it with the problem definitive resolution. Those who criticize such approach, do it for several reasons, amongst which the fact that such procedure requires a longer surgical time and causes a large dissection of a generally healthy nasal cavity.
The use of endoscopic techniques for the epistaxis surgical management has confirmed a major efficacy, a lower rate of complications and less discomfort to the patient when compared to the conservative treatment. In spite of being onerous, the endoscopic surgical treatment effectiveness and safety have been improving the method cost-benefit ratio. It's critical to remark, however, the importance of the arterial localization anatomic knowledge during intranasal surgeries. Results obtained in previous works show that about 18% of the posterior epistaxis come from ethmoidal territory and in the cases of failure of surgical treatment, the main reason is the non-identification of such origin. In our study, out of the 10 patients operated, 7 cases presented previous ligation of the sphenopalatine a. branches with new episode of bleeding in the postoperative and need for cauterization of the anterior ethmoidal a.
CONCLUSIONThe endoscopic approach for the treatment of epistaxis coming from anterior Ethmoidal artery was proven to be safe and efficient in the cases presented.
BIBLIOGRAPHICAL REFERENCES1. Ugena RE, Ruiz TG, Dominguez AJ, Claver CF, Rivero PV, Huelva BA. Utilidad del tratamiento quirúrgico de la epistaxis grave mediante abordaje endoscópico de las arterias esfenopalatina y etmoidal anterior. Acta Otorrinolaringol Esp. 2006, 57(5):228-34.
2. Hernandez VJ, Ordóñez OLE. Comparación del manejo quirúrgico versus no quirúrgico em pacientes com epistaxis posterior. Acta Otorrinolaringol Esp. 2006, 57(1):41-6.
3. Ruiz TG, Ugena RE, Palomino GA, Hernandez PCG, Santos MME, Huelva BA. Aspectos prácticos sobre el tratamiento endoscópico de la epistaxis. Acta Otorrinolaringol Esp. 2006, 57(9):394-400.
4. Araújo Filho BC, Weber R, Pinheiro Neto CD, Lessa MM, Voegels RL, Butugan O. Anatomia endoscópica da artéria etmoidal anterior: estudo de dissecção em cadáveres. Rev Bras Otorrinolaringol. 2006, 72(3):303-8.
5. Floreani SR, Nair SB, Switajewski MC, Wormald PJ. Endoscopic Anterior Ethmoidal Artery Ligation: a Cadaver Study. Laryngoscope. 2006, 116(7):1263-7.
6. Moon HJ, Kim HU, Lee JG, Chung I, Yoon JH. Surgical Anatomy of the Anterior Ethmoidal Canal in Ethmoid Roof. Laryngoscope. 2001, 111(5):900-4.
7. Lee WC, Ming Ku PK, van Hasselt CA. New Guidelines for Endoscopic Localization of the Anterior Ethmoidal Artery: A Cadaveric Study. Laryngoscope. 2000, 110(7):1173-8.
8. Pletcher SD, Metson R. Endoscopic Ligation of the Anterior Ethmoid Artery. Laryngoscope. 2007, 117(2):378-81.
9. Graham SM, Nerad JA. Orbital Complications of Endoscopic Sinus Surgery Using Powered Instrumentation. Laryngoscope. 2003, 113(5):874-8.
10. Fonseca AS, Vinhaes E, Boaventura V, Andrade NA, Dias LS, Medeiros V, Coifman F. Tratamento cirúrgico de nasoangiofibroma sem embolização. Rev Bras Otorrinolaringol. 2008, 74(4):583-7.
11. Garcia RID, Cecatto SB, Costa KS, Veiga Jr F, Uvo IP, Rapoport PB. Síndrome de Rendu-Osler-Weber: tratamento clínico e cirúrgico.Rev Bras Otorrinolaringol. 2003, 69(4):577-80.
1. Otorhinolaryngologist at the Hospital Cajuru - PUCPR. Otorhinolaryngologist of the ORL Service of PUC PR - Hospital Cajuru and Santa Casa de Misericórdia de Curitiba.
2. Head Professor of the Otorhinolaryngology Discipline of PUC PR. Head of the Otorhinolaryngology Service at PUC PR.
3. Assistant Professor of the ORL Discipline of PUC PR. Preceptor Doctor of the ORL Residence of PUC PR.
4. Resident Doctor in ORL PUCPR.
Institution: Serviço de ORL da PUC PR. Santa Casa de Misericórdia de Curitiba - Hospital Universitário Cajuru. Curitiba / PR - Brazil.
Mail address:
Carlos Augusto Seiji Maeda
Avenida Desembargador Motta, 2365 - Apto. 133
Curitiba / PR - Brazil - Zipe code: 80420-190
Fax: (+55 41) 3222-1071
E-mail: carlos_maeda@hotmail.com
Article received on October 06 2008.
Accepted on May 10 2009.