INTRODUCTIONThe larynx cartilaginous tumors are uncommon and comprise 1% of the cartilaginous tumors (1-7). The literature review reports the first descriptions made by Travers e Heusinger (4) in 1916 and so far less than 250 cases have been described, which represent 72% of chondromas and 28% of chondrosarcomas (2,5).
Chondroma, the most common benign tumor, is more common in the cricoid cartilage (75%) with incidence of 0.07-0.2% manifesting generally with dysphonia, slow progression upper respiratory passages obstruction, dyspnea and dysphagy, prevailing between the 3rd and 7th decades of life and more common in the male sex (3:1) (2,4,6,8). The most frequent location is the cricoid cartilage rear part (9,10-15).
They present with slow growth, with local aggressivity and recurrence trends (2). They are less aggressive in the larynx than in other sites and cervical remote metastases are uncommon (8.5%) (3). The symptomatology depends on the original location and the tumor extension. Dysphonia and dyspnea are frequent in the cricoid cartilage lesions, and dysphagy occurs in the growth towards the hypopharynx (15).
The chondromas differential diagnosis includes chondrometaplasia and low grade chondrosarcoma (12). As for the etiopathogenesis, in some cases we may observe cervical rachimedular trauma and vertebral instability prior to the clinical picture (4).
The neck physical exam reveals modular lesion to palpation upon prior location of the tumor and the submucous mass laryngoscopy in a rear or posterolateral portion of the subglottic area (4,10,15).
Today, with its low incidence, the experiences are limited and the knowledge tends to be limited. The objective of this study is to report a case of chondroma of the cricoid cartilage, its therapeutic management and the literature review, aiming at cooperating with the understanding of its uncommon types of tumors.
CASE REPORT21-years-old, male, white patient was attended in a private clinic with complaint of a nodular lesion in the frontal cervical region, realized for about 2-3 months, of slow and progressive growth, without other symptoms or history, in February 2002. Upon physical exam, we confirmed the formation of a hardened consistency at the cricoid cartilage level, painless, mobile to deglutition, without other masses or increased lymph nodes. The indirect laryngoscopic exam didn't confirm any lesion in the oropharynx, supraglottis, glottis or the subglottis visible part.
The computerized tomography confirmed hyperdense, well circumscribed lesion with a small calcified area more prominent in the cricoid cartilage frontal and lower portion at the left of the medium line (Picture 1).
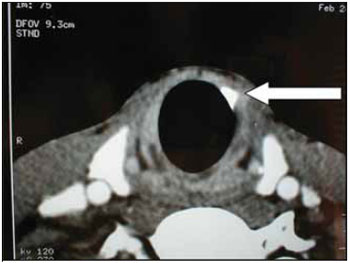
Picture 1. Computerized Tomography - Chondroma in Cricoid Cartilage.
We performed modified partial laryngectomy with resection of cricoid hemicartilage, thyroid hemicartilage and the first tracheal ring as margins. We identified and preserved previously the ipsilateral lower laryngeal nerve up to its entry in the cricopharyngeal muscle (Picture 2). The reconstruction was made through a prethyroidean muscle piece with thyroid cartilage pericondrium and tracheostomy of the suture protection. The patient evolved without intercurrences and received hospital discharge on the sixth postoperative day.

Picture 2. Intraoperative - Partial Modified Laryngectomy.
In the evolution, the patient presented with left vocal cord temporary paresis with return to the normal function in 40 days, in which the tracheostomy was removed without other complications and sequels.
Upon anatomopathological exam, the size of the tumor lesion was of 1.1 cm, and it atypically developed in the cricoid cartilage frontal region in its frontal and lateral cavities with free margins, and revealed a single pattern homogeneous structure, with low cellularity, no more than 30 or 40 cores per field, small cores and with low mitosis figures. The diagnosis was of chondroma without malignancy signs, with calcification focus in a whitish tissue, contiguous to the frontal surface of the cricoid cartilage (Picture 3 and 4).
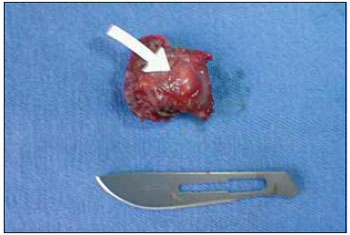
Picture 3. Surgical Piece - Chondroma in Cricoid Cartilage.

Picture 4. Chondroma Histology - Low cellularity in homogeneous half matrix.
In the service follow-up, performed with physical exam and computerized tomography at 6-month intervals, the patient didn't present with recurrences, and in the last follow-up consultation, in March 2008, he showed no evidence of the disease.
DISCUSSIONThe literature reveals an average of incidence of 65 years of age, and it's more frequent in the male sex in a proportion of 3:1 (10,11). Wang et al (7) presented an atypical case of a female patient with chondroma in the cricoid cartilage membrane frontal portion, as a cervical mass. Previous works (2-4,6,8-15) revealed that the main symptomatology is dysphonia, followed by dysphagy and dyspnea, which was not observed in this study; however, Olsen et al (12) presented two cases with salivation restriction initial picture and other two cases with limitation of the cricoid cartilage activity limitation.
Guillem et al (1) reported a case operated by an upper mediastinal symptomatic mass, with benign chondroma histopathological exam initially diagnosed without any malignancy criterion, developed from the cricoid cartilage. The blades subsequent review revealed low malignancy grade chondrosarcoma responsible for the death, and indicated the need for chondromas resection for their malignancy potential.
Nakayama et al (9) reported the case of a 7-year-old patient with clavicular metastases after laryngeal chondrosarcoma, which then evolved with cervical, pulmonary metastases and metastasis in the vertebral body. The anatomopathological exam identified the low grade chondrosarcoma transformation into an undifferentiated one (possibly the first one to be reported in a literature review of 20 cases of chondrosarcomas with remote metastases), and the differentiation grade correlates directly with the presence of remote metastases.
The computerized tomography is the complementary choice exam (4,6,9-15), and it may reveal respiratory commitment, which was not observed in this case. This statement of hyperdense well circumscribed and calcification lesion, a characteristic statement of chondromas (10,13,14), was similar to that of Wang et al (6); however the rear lateral location (1-6,8) was not identified in this report (frontal and lateral). There wasn't either a relationship between the calcification radiographic statement with the anatomopathological diagnosis. The magnetic resonance was not used in this study due to the low sensitivity to calcification (1-14); however it could be used, since it delimits the tumor extension in other tissues for its contrasted resolution in soft tissues.
Guillem et al (1) and Wang et al (7) emphasize the use of fine-needle aspiration biopsy for the cervical masses differential diagnosis, with occasional difficult performance because of the chondroma firm nature, and it wasn't performed in this case report due to the small size of the tumor; nevertheless even if we did it couldn't offer a prove of malignancy (13,14).
The cricoid cartilage tumor frontal and lateral location as described in this study, uncommon according to the literature reviewed (1-15), conditions its atypical clinical presentation as a cervical lesion without symptomatology, which is not observed in most cases where there is dysphonia, dysphagy and dyspnea, due to the more common rear and lateral location.
According to the literature, the treatment must be primarily surgical (5,6,11-15), where radiotherapy and chemotherapy are not suitable as the primary therapy, and play a secondary role. Harwood et al (13) described the use of radiotherapy in cases of lesions deemed to be irresecable, of high grade or of margins committed to the anatomopathological exam, and chemotherapy represented a controversial role even in these cases, and may be secondary in cases of concomitant remote metastases (6,13).
The excision of the cartilage segment involved with free margins is the standard treatment (11,15), both for benign and malign tumors, and recurrence occurs in the cases treated out of this objective. In many cases the difference between chondroma and chondrosarcoma is due to recurrence, and the remote metastases are uncommon (more frequent for the lung, cervical lymph nodes, kidneys and bones) (11,14,15). In our case report, there was no evidence of recurrence in the period of six years of follow-up, which clinically characterizes the chondroma.
Wang et al (6) reported that the vocal cord paralysis finding may be an early signal of the cricoarytenoid junction involvement in cases of malignancy and when the resection involves all the cricoid cartilage the full laryngectomy is indicated. They proposed that all neoplasm containing hyaline cartilage should be considered to be chondrosarcoma until the contrary is proven (6,11), and it's the only proof of benignancy at the absence of metastasis or recurrence after a variable period of time of follow-up or its entire lesion exam appearance.
The distinction between the low grade chondroma and chondrosarcoma is considered difficult in larynx cartilaginous tumors, probably it cannot be done, and it's necessary the entire piece exam for the diagnosis (9,11). The chondrosarcomas differ from the chondromas for they present major size lesions (exceeding 3 cm), typically in adults, with slow and lobular growth histological pattern, invading the adjacent tissues, with nuclear pleomorphism, polychromasia and binuclear shape (11,12,13), different findings of this case report.
Wang et al (7) propose a new classification that divides the cartilaginous tumors by malignancy into low, intermediate and high spectrum. However, this classification merely anatomopathological does not take into account these tumors clinical evolution, and other criteria are required to indicate, in certain cases, the surgical treatment radicalism.
According to Thomé (5), in cases of low grade malignancy chondromas or chondrosarcomas, the follow-up suggested that the initial surgical approach and the prognosis do not depend on the malignancy prior diagnosis and the definite histopathological distinction and that the recurrence managed with rescue surgery has no adverse impact on survival. In this report we agree with Baatenburg et al (15), in whom the treatment must be primarily surgical, but particularized for each case, where the surgical extension will obviously depend on the location and size of the cricoid cartilage tumor, and it may be adopted up to the trachea autotransplantation, by ensuring adequate margins. In certain patients in whom the surgical extension indicates full laryngectomy, other secondary treatment modalities may be adopted, aiming at the larynx preservation, since the type of surgical treatment will not affect the prognosis and only in the follow-up we will know whether the chondroma was actually chondrosarcoma.
The long-term follow-up is necessary in these patients with chondroma for the early detection of recurrences and, if there are any, the chondroma initially diagnosed could be the low grade chondrosarcoma not histologically detected (11,12,15).
In this case report, the treatment was carried out according to the literature, with adequate clinical and radiologic follow-up, and there hasn't been any evidence of recurrence or remote metastasis so far, in spite of the short time of follow-up considered for these tumors.
FINAL COMMENTSThis case report agrees with the literature regarding the surgical treatment of the chondroma of the cricoid cartilage. Due to the atypical location of the tumor found, there has been disagreement with the clinical presentation as for the symptomatology described in the literature. Other reports are required for the understanding of the natural evolution of this disease, and the resulting accumulation of experience could guide treatment protocols of these uncommon tumors of cricoid cartilage.
BIBLIOGRAPHICAL REFERENCES1. Guillem P, Porte H, Copin MC, Chevallier D. A case of giant chondrossarcoma of the cricoid cartilage presenting as a superior mediastinal tumor. Eur J Cardiothorac Surg. 1998, 14(5):520-2.
2. Polo I, Laborda J M, Alemán O, Burgos A, Talavera J, Trigueros M. Cartilaginous tumors of the larynx. A report of 3 cases. An Otorrinolaringol Ibero Am. 1998, 25(1):65-75.
3. Mata Castro N, Vega Carrasco M C, Saucedo Díaz G, Vergara Trujillo J, Veja MF. Cartilaginous tumors of the cricóide: imaging diagnosis. A case report. Acta Otorrinolaringol Esp. 1997, 48(3):247-50.
4. Verhulst J, Gal M, Carles D, Saurel J, Teixeira SM: Devars F, Traissac L. Les condromes et chondrosarcome du larynx: à propôs de 4 observations. Rev Laryngol Otol Rhinol (Bord). 1996, 117(3):183-8.
5. Thomé R, Thomé DC, de la Cortina RA. Long-term follow-up of cartilaginous tumors of the larynx. Otolaryngol Head neck Surg. 2001, 124(6):634-40.
6. Wang SJ, Borges A, Lufkin RB, Sercarz JA, Wang MB. Chondroid tumors of the larynx: computed tomography findings. Am J Otolaryngol. 1999, 20(6):379-82.
7. Wang J, Heffner DK, Venegas R, French SW. Atypical chondroma of the cricoide cartilage: fine-needle aspiration cytologic and histopathologic findings. Diagn Cytopathol. 1999, 20(3):164-6.
8. Browne JD. Management of nonnepidermoid cancer of the larynx. Current concepts in laringeal cancer II. 1997, 30(2):215-29.
9. Nakayama M, Hafez G, Brandemburg J. Dediferentiated chondrossarcoma of the larynx with regional and distant metastases. Ann Otol Rhinol Laryngol. 1993, 102:785-791.
10. Burggraaff B, Weinstein G. Imaging case study of the month Chondrosarcoma of the larynx. Ann Otol Rhinol Laryngol. 1992, 101: 183-184.
11. Devaney KO, Ferlito A, Silver CE. Clinicopathological consultation Cartilaginous tumors of the larynx. Ann Otol Rhino Laryngol. 1995, 104:251-255.
12. Lewis JE, Olsen KD, Inwards CY. Cartilaginous tumors of the larynx: clinicopathologic review of 47 cases. Ann Otol Rhino Laryngol. 1997, 106: 94-100.
13. Harwood AR, Krajbich JI, Fornasier VL. Radiotherapy of chondrosarcoma of bone. Cancer. 1980, 45:2769-2777.
14. Kambic V, Zargi M, Gale N. Laryngeal chondrossarcoma: is conservative surgery adequate treatment?. The Journal of Laryngology and Otology. 1989, 103:970-972.
15. Baatenburg de Jonq RJ, van Lent S, Hogendoorn PC. Chondroma and Chondrossarcoma of the larynx. Curr Opin Otolaryngol Head Neck Surg. 2004, 12(2):98-105.
1. Master's degree-FMUSP; TCBC-SP. Assistant of Head and Neck Surgery of the Head and Neck Surgical Service of the Hospital Beneficência Portuguesa de São Paulo.
2. Resident In Graduation in Otorhinolaryngology for the Otorhinolaryngology Service "Ivan Fairbanks Barbosa" of the Hospital Beneficência Portuguesa de São Paulo.
3. Trainee In Graduation of the Head and Neck Surgery Service "Jorge Fairbanks Barbosa" of the Hospital Beneficência Portuguesa de São Paulo.
Institution: Serviços de Cirurgia de Cabeça e Pescoço Dr. Jorge Fairbanks Barbosa e de Otorrinolaringologia Dr. Ivan Fairbanks Barbosa do Hospital Beneficência Portuguesa de São Paulo. São Paulo / SP - Brazil
Mail address:
Giulianno Molina de Melo
Rua Dr. Luis Migliano, 761 Apto 84-B - Morumbi
São Paulo / SP - Brazil - Zip code: 05711-001
Telephones: (+55 11) 3283-4591 and 3683-2401 - Fax: (+55 11) 3683-2401 and 3283-4591
E-mail: giulianno_molina@hotmail.com
Article received on November 24, 2007.
Approved on May 24, 2008.